Faecal incontinence in the era of sacral neuromodulation
DOI: https://doi.org/https://doi.org/10.57187/s.4298
Sami Hosaria,
Matthias Turinaa,
Michaela Ramsera
a Department of Visceral Surgery and Transplantation, University Hospital Zurich, Zurich,
Switzerland
Summary
Faecal incontinence is a debilitating
condition that significantly affects an individualʼs quality of
life. Accurate assessment and a thorough understanding of the underlying aetiology
are crucial in determining the appropriate management approach. Conservative
management strategies, including dietary modifications, pelvic floor exercises
and biofeedback therapy are the first therapeutic steps. If these measures are
not effective, patients should be referred to a specialised pelvic floor centre
for further treatment evaluations. With the latest updates on national and
international guidelines, this review aims to provide a comprehensive overview
of current best practices in the management of faecal incontinence, with a
particular focus on the role of sacral neuromodulation.
Epidemiology and definition
Faecal incontinence is a symptom and is defined
as the recurrent uncontrolled passage of faecal material for at least 3 months
according to the Rome IV definition. The prevalence is estimated to be around
10–15% of the adult population, with a higher incidence in women and the
elderly [1, 2]. The
terminology differentiates between faecal, flatus and mucus incontinence, and
collectively refers to them as anal incontinence.
The pathophysiology of faecal incontinence
is multifactorial and can involve sphincter weakness or injury, impaired rectal
sensation or decreased compliance of the rectal reservoir [3]. It is the
long-term consequence that occurs as a symptom of various pre-existing diseases
or traumatic lesions,
usually years after the initial event, such as obstetric trauma, haemorrhoid
resection surgery or rectal surgery [4]. The most common causes include episiotomy
or perineal tears with
lesion of the anal sphincter during childbirth, impaired neurological function
from conditions like stroke or spinal cord injury, and age-related degenerative
changes in the sphincter muscles and rectal compliance [5].
Physiology of human defecation
The process of human defecation consists of
four coordinated and sequential stages: the basal phase, the pre-expulsive
phase, the expulsive phase and the end phase. These phases work in an
orchestrated manner to facilitate the controlled expulsion of faeces.
The basal phase is characterised by contraction
of the internal anal sphincter. Continence is maintained through a predominant
retrograde activity pattern in the rectosigmoid region [6]. As the rectum fills, the
pre-expulsive phase begins, triggering the
rectoanal inhibitory reflex, which relaxes the internal anal sphincter,
allowing for afferent sensory sampling of rectal contents [7]. This relaxation is
mediated by the autonomic nervous system, with
sympathetic nerves maintaining sphincter contraction and parasympathetic nerves
inducing relaxation. The expulsive phase involves voluntary relaxation of the
external anal sphincter and pelvic floor, aided by increased abdominal
pressure, leading to expulsion. This activity is coordinated by the pontine
nuclei in the brainstem. Finally, the end phase restores anal sphincter tone
and pelvic floor relaxation. For the purposes of
this review, faecal incontinence is defined as the
inability to defer defecation, i.e. to revert from the pre-expulsive to the basal
phase, due to an underlying disorder of the afferent sensory pathways, the efferent
motor pathways from the rectum – which appears to be the main pacemaker – or
the sphincter musculature [7, 8].
Conservative management options
Recent clinical practice guidelines from
leading national and international societies, such as the European Society of
Coloproctology (ESCP), the American Society of Colon and Rectal Surgeons
(ASCRS) and the International Continence Society, have updated their
recommendations with broad commonalities on the assessment and management of faecal
incontinence. These guidelines universally advocate for a conservative
first-line approach involving pelvic floor physiotherapy, optimisation of bowel
function and stool consistency, and pharmacological interventions. However,
guidelines also recognise that the specific treatment algorithms recommended
are generally based on low-level evidence. For the initial management of faecal
incontinence, a stepwise approach is recommended. First and foremost, the
condition needs to be objectively assessed, which can often be accomplished
through a simple history-taking and digital rectal examination, without the
need for sophisticated technology [4]. The Wexner Score, a validated
questionnaire, can be used to quantify the severity of the condition [9]. It
gives information on the frequency of faecal incontinence with liquid or solid
faeces, measurements taken and the impact on quality of life.
Faecal incontinence is a prevalent and
debilitating condition that can substantially diminish an individualʼs
quality of life. It is also a stigmatised disorder, where healthcare providers
must proactively enquire about symptoms, as patients often do not voluntarily
disclose this sensitive issue [10]. Maintaining continence relies on mobility,
mental capacity, manual dexterity and motivation, and a multidisciplinary and
holistic approach is often required to address this distressing problem [11]. A comprehensive
assessment is crucial in establishing the
underlying aetiology and determining the appropriate treatment plan [2].
Conservative management measures include
dietary modifications, pelvic floor muscle training, biofeedback therapy, and
the use of medications or devices to manage incontinence [5]. Dietary changes, such
as increasing fibre intake or avoiding
certain foods that may contribute to loose stools, can help improve stool
consistency and reduce the severity of incontinence. Pelvic floor muscle
training under the guidance of a specialised physiotherapist can strengthen the
muscles responsible for maintaining continence and improve the overall function
of the pelvic floor [3]. The pelvisuisse website (https://www.pelvisuisse.ch/) gives
an overview of certified physiotherapists.
Psyllium and fibre supplementation
Soluble fibre supplements, such as
psyllium, are a common first-line treatment for faecal incontinence. Increasing
the bulk and consistency of the stool through fibre intake can enhance rectal
sensation and facilitate more controlled defecation, thereby improving
continence. However, not all fibre sources are equally effective. A randomised
trial showed that psyllium yielded the greatest reduction in incontinence
episodes, with a 51% decrease, compared to a 20% decrease with gum arabic and
only an 11% decrease with placebo. Conversely, carboxymethylcellulose was even found
to increase faecal incontinence [12].
Loperamide and antidiarrhoeal medications
The evidence suggests that loperamide, an
antidiarrhoeal medication, may be more effective than psyllium fibre
supplementation for managing faecal incontinence. A randomised trial [13] found
a statistically similar reduction in incontinence episodes of 59% with loperamide
vs 51% with
psyllium (n = 80, p = 0.18). Additionally,
the authors reported that the adverse effects profile of loperamide appears to
be more favourable, with patients reporting less bloating or abdominal pain
compared to fibre supplementation. However, the loperamide group did experience
more obstipation as a side effect.
Education and lifestyle modifications
Educating patients on the underlying
pathophysiology of faecal incontinence and empowering them with practical
strategies can significantly improve outcomes. In countries like Denmark, this
consulting and education is performed by nurse-led clinics. A trial performed
in the USA compared patient education + placebo with patient education + loperamide
[14]. The addition of loperamide to an educational programme led to a 73%
reduction in faecal incontinence episodes per day vs a 59% reduction with
education alone. But the main takeaway was that all groups improved,
highlighting the importance of education, lifestyle modifications and patient
engagement as essential components of a comprehensive management approach.
Interventional and surgical treatment options
In cases where conservative measures prove
insufficient, various surgical options may be considered. Before the
consideration of surgery, further diagnostics are recommended to determine the
underlying aetiology [15].
Specialised diagnostic testing like
anorectal manometry, rectal sensory testing, endoanal ultrasound and MRI
defecography are recommended to objectively understand aetiology and underlying
reasons of faecal incontinence [16].
The evaluation of surgical options then
includes all findings of the above diagnostics. If an anatomical abnormality or
a significant dynamic structural evacuation disorder is found, such as rectal
prolapse or rectocele, the respective surgical correction should be considered.
Furthermore, the degree of sphincter defect plays an important role in
decision-making and therapeutic options. For a defect greater than 180 degrees,
the surgical options include sphincteroplasty with or without vaginal and
perineal reconstruction, sacral neuromodulation or creation of a colostomy. For
a 90–180 degree defect, the options are sacral neuromodulation, colostomy and
sphincteroplasty. For a defect less than 90 degrees, only sacral
neuromodulation and colostomy are recommended [16].
Over the past few decades and also in
comparison to previous guidelines, recommendations for surgery have undergone
significant changes. Procedures like dynamic graciloplasty and implantation of
artificial or magnetic anal sphincters [17] are no longer recommended or have even
been withdrawn from the market [16]. Emerging modalities such as the
Gatekeeper/Sphinkeeper and bioinjectables have very limited data, and thus are
not represented in current clinical practice guidelines. This has left
clinicians with a relatively narrow set of surgical options to treat faecal
incontinence. However, the following surgical options have gained importance and growing
evidence supporting their effectiveness in managing faecal incontinence [18–21].
Sphincteroplasty
Sphincter reconstruction, a surgical option
for faecal incontinence caused by sphincter defects, may be indicated for
patients with structural defects, such as obstetric trauma [22] repair. Long-term
outcomes of sphincter repair are variable, with various groups reporting a high
recurrence rate of faecal incontinence within 80 months and more than 76% with
treatment failure or only a small improvement of faecal incontinence [23–25]. While
initial outcomes can be positive, long-term results show that this
effectiveness decrease over time [24, 26]. The average length of time before
this decline becomes apparent can vary, but after five years patients typically
recognise a subjective reduction of the initially gained continence. In our
experience, only patients with a very recent sphincter lesion event benefit
from a sphincter repair.
Sacral neuromodulation
Sacral neuromodulation is a surgical
procedure that involves the implantation of a device that stimulates the sacral
nerves, which can help improve bowel function and control [27]. Numerous
studies have demonstrated the effectiveness of sacral neuromodulation in
managing faecal incontinence, with significant improvements in symptom severity
and quality of life [28]. In particular, long-term data on this approach are promising
[29]. Sacral neuromodulation not yet fully understood but aims to modulate the
neuronal control of bowel function and thereby improve faecal incontinence [27,
30, 31]. Electrical modulation is believed to enhance interoception and improve
the deferment mechanisms [32]. Furthermore, sacral neuromodulation is emerging
for new indications: it has been shown to also improve chronic constipation [33,
34], low anterior resection syndrome (LARS) [35–38] and signs of rectal
evacuation disorders [34, 39–41]. Therefore, the benefits of sacral
neuromodulation in the management of faecal incontinence have become
increasingly recognised, leading to its inclusion as a recommended surgical
option in the newest clinical practice guidelines.
In recent years, many publications have
sought to re-evaluate treatment strategies and the value of other surgical
interventions in the context of the growing recognition of the benefits of
sacral neuromodulation. This emerging concept has been dubbed “the era
of sacral neuromodulation”, which reflects the increasing importance
and acceptance of this therapy as a key approach for managing faecal
incontinence.
Sacral neuromodulation therapy involves a
staged surgical approach, providing an opportunity to assess its efficacy
before definitive implantation.
In the first stage, often referred to as
the test phase, the electrodes, which are connected to a temporary external
stimulator, are placed near the sacral nerve. The patient monitors the
effectiveness of this therapy by keeping a diary of their symptoms and faecal
incontinence episodes during the trial period. This stage offers the benefit of
assessing the patientʼs response, allowing for the optimisation of electrode selection,
stimulation intensity and frequency. If significant symptom improvement is
observed, a second surgery is performed to implant the device subcutaneously [42,
43].
In Switzerland, sacral neuromodulation implantation
is limited to designated centres that have been certified for sacral neuromodulation
implantation. At the authors’ institution, sacral neuromodulation was
introduced in 2004, and since then more than 100 implantations have been
performed.
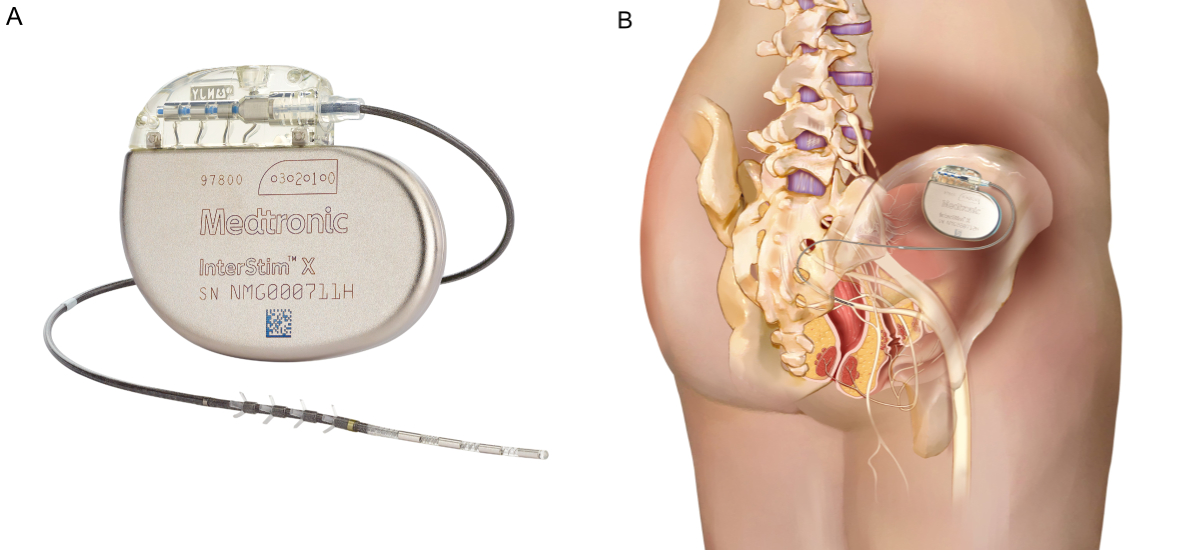
Figure 1Sacral neuromodulation device –
Medtronic InterStim System. (A) Medtronic InterStim™ X implantable pulse
generator with lead for sacral nerve stimulation. (B) Anatomical placement near
the S3 sacral nerve for modulating bowel and bladder function. With kind
permission of Medtronic Schweiz AG.
Colostomy
When all other conservative and surgical
treatment options have been exhausted, a colostomy may be considered as a final
resort for patients with severe and debilitating faecal incontinence. For
individuals with severe faecal incontinence and recurrent symptoms despite
maximal medical therapy and failure of surgical options, a diverting stoma
represents a viable option that can effectively restore continence and return
independence.
Conclusion
Faecal incontinence represents a
significant and frequently debilitating condition that necessitates a
comprehensive approach for effective management. Key steps in managing faecal
incontinence include the early identification of high-risk individuals, such as
those with childbirth-related trauma or neurological disorders. Proactive
screening, which involves actively asking about symptoms, is important. Utilising
tools like the Wexner Score helps quantify the severity and guide the selection
of appropriate management strategies. The initial management should focus on
conservative interventions, including dietary modifications, as well as
improving stool consistency with psyllium and/or medications such as
loperamide.
When conservative treatments prove
insufficient, referral to a specialised pelvic floor centre is recommended for
further diagnostics and evaluation for surgical management.
Among the available surgical options, sacral neuromodulation has emerged as a
method providing symptom control and quality of life improvement. The recognised
efficacy of sacral neuromodulation has led to its inclusion in clinical
practice guidelines, positioning it as a pivotal therapy for patients who do
not respond adequately to first-line treatments.
Sami Hosari
Department of Visceral Surgery and Transplantation
University Hospital Zurich
CH-8091 Zurich
Sami.Hosari[at]usz.ch
References
1. Whitehead WE, Simren M, Busby-Whitehead J, Heymen S, van Tilburg MA, Sperber AD, et
al. Fecal incontinence diagnosed by the Rome IV criteria in the United States, Canada,
and the United Kingdom. Clin Gastroenterol Hepatol. 2020 Feb;18(2):385–91. doi: https://doi.org/10.1016/j.cgh.2019.05.040
2. Findlay JM, Maxwell-Armstrong C. Current issues in the management of adult faecal
incontinence. Br J Hosp Med (Lond). 2010 Jun;71(6):335–40. doi: https://doi.org/10.12968/hmed.2010.71.6.48446
3. Maslekar S, Gardiner A, Maklin C, Duthie GS. Investigation and treatment of faecal
incontinence. Postgrad Med J. 2006 Jun;82(968):363–71. doi: https://doi.org/10.1136/pgmj.2005.044099
4. Ahmad M, McCallum IJ, Mercer-Jones M. Management of faecal incontinence in adults.
BMJ. 2010;340:c2964. doi: https://doi.org/10.1136/bmj.c2964
5. Barrie M. Nursing management of patients with faecal incontinence. Nurs Stand. 2018 May;33(2):69–74.
doi: https://doi.org/10.7748/ns.2018.e11167
6. Lin AY, Varghese C, Paskaranandavadivel N, Seo S, Du P, Dinning P, et al. Faecal incontinence
is associated with an impaired rectosigmoid brake and improved by sacral neuromodulation.
Colorectal Dis. 2022 Dec;24(12):1556–66. doi: https://doi.org/10.1111/codi.16249
7. Heitmann PT, Vollebregt PF, Knowles CH, Lunniss PJ, Dinning PG, Scott SM. Understanding
the physiology of human defaecation and disorders of continence and evacuation. Nat
Rev Gastroenterol Hepatol. 2021 Nov;18(11):751–69. doi: https://doi.org/10.1038/s41575-021-00487-5
8. Cerdán J, Cerdán C, Jiménez F. Anatomofisiología de la continencia y la defecación
[Anatomy and physiology of continence and defecation]. Cir Esp. 2005 Dec;78(3 Suppl
3):2–7. doi: https://doi.org/10.1016/S0009-739X(05)74637-6
9. Norton C, Thomas L, Hill J; Guideline Development Group. Management of faecal incontinence
in adults: summary of NICE guidance. BMJ. 2007 Jun;334(7608):1370–1. doi: https://doi.org/10.1136/bmj.39231.633275.AD
10. Brown HW, Guan W, Schmuhl NB, Smith PD, Whitehead WE, Rogers RG. If we don’t ask,
they won’t tell: screening for urinary and fecal incontinence by primary care providers.
J Am Board Fam Med. 2018;31(5):774–82. doi: https://doi.org/10.3122/jabfm.2018.05.180045
11. Goodman C, Norton C, Buswell M, Russell B, Harari D, Harwood R, et al. Managing Faecal
INcontinence in people with advanced dementia resident in Care Homes (FINCH) study:
a realist synthesis of the evidence. Health Technol Assess. 2017 Aug;21(42):1–220.
doi: https://doi.org/10.3310/hta21420
12. Bliss DZ, Savik K, Jung HJ, Whitebird R, Lowry A, Sheng X. Dietary fiber supplementation
for fecal incontinence: a randomized clinical trial. Res Nurs Health. 2014 Oct;37(5):367–78.
doi: https://doi.org/10.1002/nur.21616
13. Markland AD, Burgio KL, Whitehead WE, Richter HE, Wilcox CM, Redden DT, et al. Loperamide
versus psyllium fiber for treatment of fecal incontinence: the fecal incontinence
prescription (Rx) management (FIRM) randomized clinical trial. Dis Colon Rectum. 2015 Oct;58(10):983–93.
doi: https://doi.org/10.1097/DCR.0000000000000442
14. Jelovsek JE, Markland AD, Whitehead WE, Barber MD, Newman DK, Rogers RG, et al.; National
Institute of Child Health and Human Development Pelvic Floor Disorders Network. Controlling
faecal incontinence in women by performing anal exercises with biofeedback or loperamide:
a randomised clinical trial. Lancet Gastroenterol Hepatol. 2019 Sep;4(9):698–710.
doi: https://doi.org/10.1016/S2468-1253(19)30193-1
15. George BD. Anal and perianal disorders. Medicine. 2011;39(2):84–9. doi: https://doi.org/10.1016/j.mpmed.2010.11.011
16. Assmann SL, Keszthelyi D, Kleijnen J, Anastasiou F, Bradshaw E, Brannigan AE, et al. Guideline
for the diagnosis and treatment of Faecal Incontinence-A UEG/ESCP/ESNM/ESPCG collaboration.
United European Gastroenterol J. 2022 Apr;10(3):251–86. doi: https://doi.org/10.1002/ueg2.12213
17. Wexner SD, Baeten C, Bailey R, Bakka A, Belin B, Belliveau P, et al. Long-term efficacy
of dynamic graciloplasty for fecal incontinence. Dis Colon Rectum. 2002 Jun;45(6):809–18.
doi: https://doi.org/10.1007/s10350-004-6302-1
18. Katuwal B, Bhullar J. Corrigendum: Current Position of Sacral Neuromodulation in Treatment
of Fecal Incontinence. Clinics in Colon and Rectal Surgery. 2021;34(01):e1-e.
19. Jarrett ME, Mowatt G, Glazener CM, Fraser C, Nicholls RJ, Grant AM, et al. Systematic
review of sacral nerve stimulation for faecal incontinence and constipation. Br J
Surg. 2004 Dec;91(12):1559–69. doi: https://doi.org/10.1002/bjs.4796
20. Uludağ O, Melenhorst J, Koch SM, van Gemert WG, Dejong CH, Baeten CG. Sacral neuromodulation:
long-term outcome and quality of life in patients with faecal incontinence. Colorectal
Dis. 2011 Oct;13(10):1162–6. doi: https://doi.org/10.1111/j.1463-1318.2010.02447.x
21. Mellgren A, Wexner SD, Coller JA, Devroede G, Lerew DR, Madoff RD, et al.; SNS Study
Group. Long-term efficacy and safety of sacral nerve stimulation for fecal incontinence.
Dis Colon Rectum. 2011 Sep;54(9):1065–75. doi: https://doi.org/10.1097/DCR.0b013e31822155e9
22. Dudding TC, Vaizey CJ, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors,
and management. Ann Surg. 2008 Feb;247(2):224–37. doi: https://doi.org/10.1097/SLA.0b013e318142cdf4
23. Goetz LH, Lowry AC. Overlapping sphincteroplasty: is it the standard of care? Clin
Colon Rectal Surg. 2005 Feb;18(1):22–31. doi: https://doi.org/10.1055/s-2005-864072
24. Glasgow SC, Lowry AC. Long-term outcomes of anal sphincter repair for fecal incontinence:
a systematic review. Dis Colon Rectum. 2012 Apr;55(4):482–90. doi: https://doi.org/10.1097/DCR.0b013e3182468c22
25. Barisic GI, Krivokapic ZV, Markovic VA, Popovic MA. Outcome of overlapping anal sphincter
repair after 3 months and after a mean of 80 months. Int J Colorectal Dis. 2006 Jan;21(1):52–6.
doi: https://doi.org/10.1007/s00384-004-0737-7
26. Mongardini FM, Cozzolino G, Karpathiotakis M, Cacciatore C, Docimo L. Short- and long-term
outcomes of sphincteroplasty for anal incontinence related to obstetric injury: a
systematic review. Updates Surg. 2023 Sep;75(6):1423–30. doi: https://doi.org/10.1007/s13304-023-01609-1
27. Matzel KE, Stadelmaier U, Hohenberger W. Innovations in fecal incontinence: sacral
nerve stimulation. Dis Colon Rectum. 2004 Oct;47(10):1720–8. doi: https://doi.org/10.1007/s10350-004-0636-6
28. Hull T, Giese C, Wexner SD, Mellgren A, Devroede G, Madoff RD, et al.; SNS Study Group.
Long-term durability of sacral nerve stimulation therapy for chronic fecal incontinence.
Dis Colon Rectum. 2013 Feb;56(2):234–45. doi: https://doi.org/10.1097/DCR.0b013e318276b24c
29. Janssen PT, Kuiper SZ, Stassen LP, Bouvy ND, Breukink SO, Melenhorst J. Fecal incontinence
treated by sacral neuromodulation: long-term follow-up of 325 patients. Surgery. 2017 Apr;161(4):1040–8.
doi: https://doi.org/10.1016/j.surg.2016.10.038
30. Madoff RD, Parker SC, Varma MG, Lowry AC. Faecal incontinence in adults. Lancet. 2004 Aug;364(9434):621–32.
doi: https://doi.org/10.1016/S0140-6736(04)16856-6
31. Ratto C, Ganio E, Naldini G; GINS. Long-term results following sacral nerve stimulation
for chronic constipation. Colorectal Dis. 2015 Apr;17(4):320–8. doi: https://doi.org/10.1111/codi.12857
32. Dasgupta R, Critchley HD, Dolan RJ, Fowler CJ. Changes in brain activity following
sacral neuromodulation for urinary retention. J Urol. 2005 Dec;174(6):2268–72. doi: https://doi.org/10.1097/01.ju.0000181806.59363.d1
33. Sharma A, Bussen D, Herold A, Jayne D. Review of sacral neuromodulation for management
of constipation. Surg Innov. 2013 Dec;20(6):614–24. doi: https://doi.org/10.1177/1553350613475882
34. Maeda Y, Kamm MA, Vaizey CJ, Matzel KE, Johansson C, Rosen H, et al. Long-term outcome
of sacral neuromodulation for chronic refractory constipation. Tech Coloproctol. 2017 Apr;21(4):277–86.
doi: https://doi.org/10.1007/s10151-017-1613-0
35. Schwandner O. Sacral neuromodulation for fecal incontinence and “low anterior resection
syndrome” following neoadjuvant therapy for rectal cancer. Int J Colorectal Dis. 2013 May;28(5):665–9.
doi: https://doi.org/10.1007/s00384-013-1687-8
36. Pires M, Severo M, Lopes A, Neves S, Matzel K, Povo A. Sacral neuromodulation for
low anterior resection syndrome: current status-a systematic review and meta-analysis.
Int J Colorectal Dis. 2023 Jul;38(1):189. doi: https://doi.org/10.1007/s00384-023-04485-8
37. De Meyere C, Nuytens F, Parmentier I, D’Hondt M. Five-year single center experience
of sacral neuromodulation for isolated fecal incontinence or fecal incontinence combined
with low anterior resection syndrome. Tech Coloproctol. 2020 Sep;24(9):947–58. doi: https://doi.org/10.1007/s10151-020-02245-2
38. Marinello F, Fraccalvieri D, Planellas P, Adell Trapé M, Gil JM, Kreisler E, et al. Sacral
Neuromodulation in Patients With Low Anterior Resection Syndrome: The SANLARS Randomized
Clinical Trial. Dis Colon Rectum. 2024 Mar;67(3):435–47. doi: https://doi.org/10.1097/DCR.0000000000003143
39. Chan DK, Barker MA. Effective treatment of dyssynergic defecation using sacral neuromodulation
in a patient with cerebral palsy. Female Pelvic Med Reconstr Surg. 2015;21(3):e27–9.
doi: https://doi.org/10.1097/SPV.0000000000000147
40. Widmann B, Galata C, Warschkow R, Beutner U, Ögredici Ö, Hetzer FH, et al. Success
and complication rates after sacral neuromodulation for fecal incontinence and constipation:
a single-center follow-up study. J Neurogastroenterol Motil. 2019 Jan;25(1):159–70.
doi: https://doi.org/10.5056/jnm17106
41. Ganio E, Ratto C, Masin A, Luc AR, Doglietto GB, Dodi G, et al. Neuromodulation for
fecal incontinence: outcome in 16 patients with definitive implant. The initial Italian
Sacral Neurostimulation Group (GINS) experience. Dis Colon Rectum. 2001 Jul;44(7):965–70.
doi: https://doi.org/10.1007/BF02235484
42. Zbar AP. Sacral neuromodulation and peripheral nerve stimulation in patients with
anal incontinence: an overview of techniques, complications and troubleshooting. Gastroenterol
Rep (Oxf). 2014 May;2(2):112–20. doi: https://doi.org/10.1093/gastro/gou015
43. Spinelli M, Sievert KD. Latest technologic and surgical developments in using InterStim
Therapy for sacral neuromodulation: impact on treatment success and safety. Eur Urol.
2008 Dec;54(6):1287–96. doi: https://doi.org/10.1016/j.eururo.2008.01.076