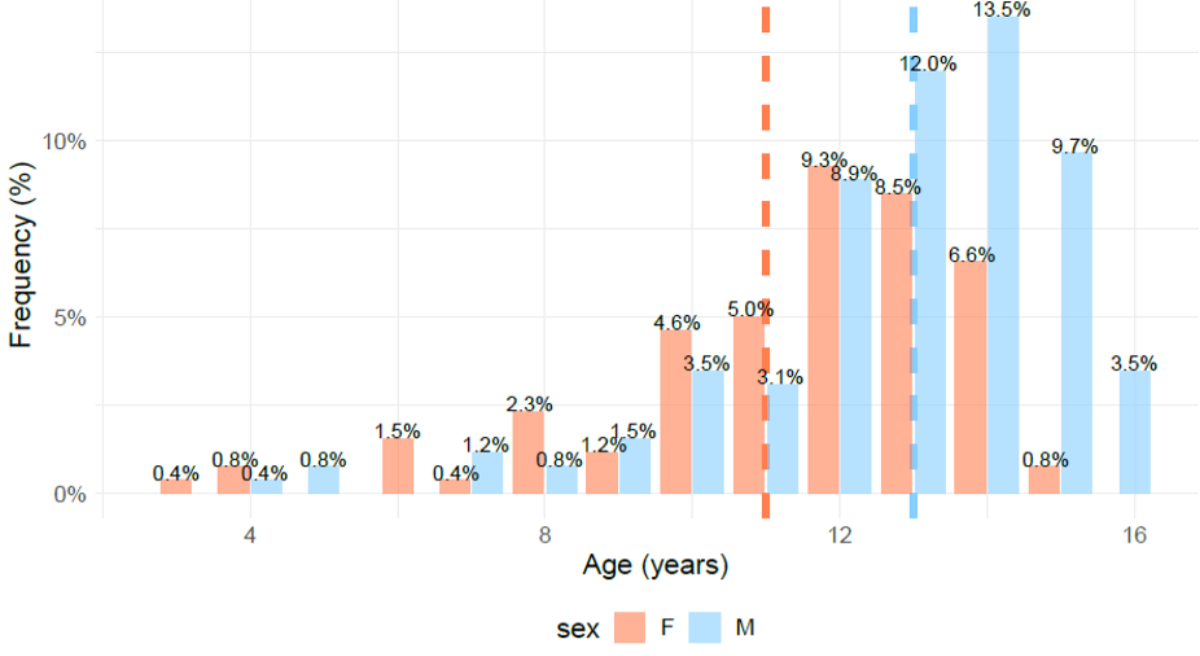
Figure 1Sex and age distribution distinguishing for pubertal status. The peak for males was at 14 years, corresponding to 13.5%. The peak for females was at 12 years, corresponding to 9.3%. F: females; M: males.
DOI: https://doi.org/https://doi.org/10.57187/s.4265
Ankle physeal fractures are a significant concern in paediatric orthopaedics due to their potential to cause premature physeal closure (PPC), which can result in complications such as bar formation, angular deformities, joint malalignment or lower-limb length discrepancies [1–3]. Knowledge about the epidemiology of physeal fractures is a starting point for understanding the risk factors for PPC and its treatment and prevention. The epidemiology of limb physeal fractures has evolved over the decades. Historical epidemiological cohorts have shown that physeal fractures accounted for 15–30% of all paediatric fractures and affected upper limbs more commonly than lower limbs, with ratios ranging from 1.6:1 to 3:1, and involving the distal tibia in 10.9% of cases [4–7]. Recent data from a national trauma database in the United States indicated that 5.7% of all limb fractures involved the physis, with 8.5% of lower-limb fractures affecting growth plates [8, 9]. In the lower limbs, the distal tibia represented the site most frequently affected (23.5%) by physeal fractures. Of all distal tibia and fibula physeal fractures in males, 73.9% occurred in boys aged 13–18; and 84.5% of those in females occurred in girls aged 9–12 [8, 9]. The divergent epidemiology of ankle physeal fractures in historical and more recent studies probably correlates with paediatric populations’ changing activities and lifestyles over the decades. Moreover, the wide range in the prevalence of PPC seen in distal tibial fractures – varying from 1% to 66.7% in the literature – could be related to differences in sample sizes across epidemiological studies and the variable distributions of fracture patterns as classified using the Salter-Harris and Dias-Tachdjian systems [4, 10–15]. Thus, it is relevant to obtain robust epidemiological data on ankle physeal fractures to improve knowledge about their distribution by fracture pattern and age, as well as their actual incidence and the impact of PPC.
The present study aimed to address gaps in the current literature by providing a large-scale, retrospective descriptive epidemiological analysis of paediatric ankle physeal fractures treated at a single university hospital centre in Switzerland. It focused on demographic distribution, seasonal trends, mechanisms of injury and fracture patterns using both the Salter-Harris and Dias-Tachdjian classification systems.
After obtaining approval from the local ethics committee (CE 2023-01624), we retrospectively reviewed all cases of paediatric patients admitted to our institution for ankle physeal fractures from 1 January 2004 to 30 April 2023. Geneva Children’s Hospital is a level I university hospital trauma centre for paediatric patients and a referral centre for the Geneva region and neighbouring areas of France. The study included patients aged up to 16 years. Patients without radiological images or medical charts, those with neurological conditions or syndromes, as well as those not able to walk were excluded.
We collected demographic data (age, sex, side of the injured ankle), injury information (date, season, mechanism of injury) and fracture patterns using the Dias-Tachdjian classification [15]. Fracture descriptions were based on conventional imaging studies using the Salter-Harris classification, and we noted whether the fractures were open or closed [14]. Patients were categorised based on pubertal status, with thresholds set at 11 years for girls and 13 years for boys. Seasonal distribution was defined with spring starting on 1 March, summer on 1 June, autumn on 1 September and winter on 1 December. The mechanisms and contexts of injuries were categorised into sports injuries, outdoor play (such as tobogganing, riding a scooter, zip-lining and trampolining), falls from a height, slips and torsions, crushing trauma, feet caught in bicycle wheels and road accidents. Length of follow-up was not considered an exclusion criterion as the study focused primarily on the diagnostic element of children’s ankle physeal fractures.
Charts with missing data were excluded, complete case analyses were carried out. Data were analysed using R software (version 4.2.2, R Development Core Team). Descriptive analyses included the mean, standard deviation (SD) and range (minimum–maximum) of continuous variables and absolute counts and percentages for categorical variables. Differences in the distributions of Salter-Harris classifications and Dias-Tachdjian injury mechanisms between female and male groups were analysed using Fisher’s exact test for dichotomous outcomes. Effect sizes and 95% confidence intervals (95% CI) were reported, and statistical significance was set at p <0.05.
The study included 259 patients with ankle physeal fractures, 152 (58.7%) of whom were male, resulting in a male–female ratio of 1.4:1. The mean age was 12.3 years (SD 2.4; range 3.5–16 years). There was a unimodal distribution of fractures in the pubertal age group, peaking at age 12 among females (9.3%) and 14 among males (13.5%) (figure 1). Most fractures occurred in pubertal patients, reaching 72.9% among females and 65.8% among males (table 1). Ankle physeal fractures more frequently affected the right ankle (54.1%). Detailed demographic data are provided in table 1, and the distribution of fractures by age and sex is illustrated in figure 1.
Figure 1Sex and age distribution distinguishing for pubertal status. The peak for males was at 14 years, corresponding to 13.5%. The peak for females was at 12 years, corresponding to 9.3%. F: females; M: males.
Table 1Demographic data. Categorical variables are described using an absolute count and a percentage.
| Females | Males | Overall | ||
| Sample size | 107 (41.3%) | 152 (58.7%) | 259 (100%) | |
| Age in years | Mean | 11.4 | 12.8 | 12.3 |
| SD | 2.4 | 2.3 | 2.4 | |
| Min–Max | 3.5–15.9 | 4.0–16.0 | 3.5–16 | |
| Pubertal status* | Prepubertal | 29 (27.1%) | 52 (34.2%) | 81 (31.3%) |
| Pubertal | 78 (72.9%) | 100 (65.8%) | 178 (68.7%) | |
| Injured ankle | Left | 48 (44.9%) | 71 (46.7%) | 119 (45.9%) |
| Season** | Winter | 31 (29.0%) | 30 (19.7%) | 61 (23.6%) |
| Spring | 24 (22.4%) | 45 (29.6%) | 69 (26.6%) | |
| Summer | 19 (17.8%) | 29 (19.1%) | 48 (18.5%) | |
| Autumn | 33 (30.8%) | 48 (31.6%) | 81 (31.3%) | |
| Injury type | Falls | 14 (13.1%) | 14 (9.2%) | 28 (10.8%) |
| Slipping | 4 (3.7%) | 3 (2.0%) | 7 (2.7%) | |
| Torsion | 6 (5.6%) | 3 (2.0%) | 9 (3.5%) | |
| Outdoor activities | 9 (8.4%) | 15 (9.9%) | 24 (9.3%) | |
| Fall from a height | 6 (5.6%) | 13 (8.6%) | 19 (7.3%) | |
| Road accidents | 11 (10.3%) | 18 (11.8%) | 29 (11.2%) | |
| Crushing trauma | 3 (2.8%) | 2 (1.3%) | 5 (1.9%) | |
| Foot caught in a bicycle wheel | 4 (3.7%) | 2 (1.3%) | 6 (2.3%) | |
| Sports | 50 (46.7%) | 82 (53.9%) | 132 (51.0%) |
* Puberty defined as age ≥11 years for females and ≥13 years for males.
** Start dates of seasons defined as 1 December for winter, 1 March for spring, 1 June for summer and 1 September for autumn.
The peak incidence of ankle physeal fractures occurred in autumn for both females (30.8%) and males (31.6%), followed by spring and winter (table 1).
Overall, 51% of fractures occurred during sports activities, with soccer and skateboarding being the most common among males. Among females, the main sports were gymnastics, followed by horse riding (table 1 and 2). The third most common cause of trauma among females was falls, whereas road accidents, especially pedestrian–car accidents, were the third cause of injury among males (table 1).
Table 2Sports types. Categorical variables are described using an absolute count and a percentage.
| Sports types | Females | Males | Overall |
| Soccer | 5 (4.7%) | 41 (27.0%) | 46 (17.8%) |
| Rugby | 1 (0.9%) | 1 (0.7%) | 2 (0.8%) |
| Volleyball | 0 | 1 (0.7%) | 1 (0.4%) |
| Basketball | 0 | 4 (2.6%) | 4 (1.6%) |
| Skateboarding | 8 (7.5%) | 14 (9.2%) | 22 (8.5%) |
| Roller skating | 2 (1.9%) | 1 (0.7%) | 3 (1.2%) |
| Gymnastics | 10 (9.3%) | 7 (4.6%) | 17 (6.6%) |
| Acrobatics | 0 | 2 (1.3%) | 2 (0.8%) |
| Parkour | 2 (1.9%) | 0 | 2 (0.8%) |
| Skiing | 3 (2.8%) | 2 (1.3%) | 5 (1.9%) |
| Snowboarding | 1 (0.9%) | 0 | 1 (0.4%) |
| Skating | 1 (0.9%) | 4 (2.6%) | 5 (1.9%) |
| Wakeboarding | 1 (0.9%) | 0 | 1 (0.4%) |
| Running | 0 | 2 (1.3%) | 2 (0.8%) |
| Climbing | 1 (0.9%) | 0 | 1 (0.4%) |
| Sledging | 3 (2.8%) | 1 (0.7%) | 4 (1.5%) |
| Horse riding | 8 (7.5%) | 1 (0.7%) | 9 (3.5%) |
| Judo | 2 (1.9%) | 0 | 2 (0.8%) |
| Trampolining | 2 (1.9%) | 1 (0.7%) | 3 (1.2%) |
Isolated physeal fractures of the distal tibia were the most common type of ankle physeal fracture (122/259, 47.1%), followed by bimalleolar fractures (117/259, 45.1%) (figure S1 in the appendix). Distal tibia transitional fractures accounted for 40.1% (122/259) of physeal fractures, with 21.6% being among females and 18.5% being among males (table 3, figure S1).
Table 3Distribution according to the Salter-Harris and Dias-Tachdjian classifications and open fractures.
| Females (n = 107) | Males (n = 152) | Overall (n = 259) | ||
| Salter-Harris classification | SH1 | 4 (3.7%) | 10 (6.6%) | 14 (5.4%) |
| SH2 | 45 (42.1%) | 87 (57.2%) | 132 (51.0%) | |
| SH3 | 29 (27.1%) | 29 (19.1%) | 58 (22.4%) | |
| SH4 | 29 (27.1%) | 26 (17.1%) | 55 (21.2%) | |
| Transitional fractures | Triplane | 19 (17.7%) | 18 (11.8%) | 37 (14.3%) |
| McFarland and Tillaux fractures | McFarland | 26 (24.3%) | 21 (13.8%) | 47 (18.1%) |
| Tillaux | 11 (10.3%) | 9 (5.9%) | 20 (7.7%) | |
| Mechanism of trauma | SI | 30 (28.0%) | 36 (23.7%) | 66 (25.5%) |
| SPF | 31 (29.0%) | 56 (36.8%) | 87 (33.6%) | |
| SER | 32 (29.9%) | 34 (22.4%) | 66 (25.5%) | |
| PEER | 12 (11.2%) | 25 (16.4%) | 37 (14.3%) | |
| Not classifiable | 2 (1.9%) | 1 (0.7%) | 3 (1.2%) | |
| Open fractures | Overall | 2 (1.9%) | 2 (1.3%) | 4 (1.6%) |
| Gustilo 1 | 1 (0.9%) | 0 | 1 (0.4%) | |
| Gustilo 2 | 0 | 1 (0.7%) | 1 (0.4%) | |
| Gustilo 3 | 1 (1.9%) | 1 (0.7%) | 2 (0.8%) | |
PEER: pronation, eversion, external rotation; SER: supination, external rotation; SI: supination, inversion; SPF: supination, plantar flexion.
Three patterns of bimalleolar fractures (117/259) were identified. There were 16 physeal fractures of both the distal tibia and fibula, 97 physeal fractures of the distal tibia (mainly Salter-Harris type II) combined with metaphyseal/diaphyseal fractures or avulsion fractures of the distal fibula, and four physeal fractures of the distal fibula combined with metaphyseal/diaphyseal fractures of the distal tibia (figure S1).
Considering the overall distribution of these fractures according to the Salter-Harris classification, Salter-Harris type II fractures were the most common (51%), involving slightly more males than females (57.2% versus 42.1%, respectively, with p <0.05) (table 4). In decreasing order, these were followed by Salter-Harris types III, IV and I at 22.4%, 21.2% and 5.4%, respectively). Salter-Harris types III and IV involved slightly higher proportions of females (table 3).
Table 4Correlations between sex, Salter-Harris classification and mechanism of injury according to the Dias-Tachdjian classification. Results are presented as n (%); p-value significance was set at p <0.05.
| Females (n = 107) | Males (n = 152) | p-value | Effect sizes | 95% confidence interval | ||
| Salter-Harris classification, n (%) | SH1 | 4 (3.7%) | 10 (6.6%) | 0.474 | 0.032 | −9.0%–3.3% |
| SH2 | 45 (42.1%) | 87 (57.2%) | 0.023* | 0.323 | −28.2%–−2.2% | |
| SH3 | 29 (27.1%) | 29 (19.1%) | 0.170 | 0.117 | −3.3%–19.3% | |
| SH4 | 29 (27.1%) | 26 (17.1%) | 0.075 | 0.198 | −1.1%–21.1% | |
| Mechanism, n (%) | SI | 30 (28.0%) | 36 (23.7%) | 0.518 | 0.026 | −7.3%–16.0% |
| SPF | 31 (29.0%) | 56 (36.8%) | 0.235 | 0.088 | −20.2%–36.8% | |
| SER | 32 (29.9%) | 34 (22.4%) | 0.220 | 0.093 | −4.2%–19.2% | |
| PEER | 12 (11.2%) | 25 (16.4%) | 0. 315 | 0.063 | −14.4%–4.0% | |
| Not classifiable | 1 (1.9%) | 2 (0.7%) | 0.759 | 0.006 | −2.5%–4.9% | |
* Result reaching statistical significance.
PEER: pronation, eversion, external rotation; SER: supination, external rotation; SI: supination, inversion; SPF: supination, plantar flexion.
By sex, the most common fracture types among females were transitional fractures (21.6%), whereas males presented more frequently with distal tibia physeal fractures combined with distal fibula metaphyseal/diaphyseal fractures or avulsions (27.8%). Open fractures were rare (1.6%), with most classified as Gustilo type 3 (table 3).
According to the Dias-Tachdjian classification (figure S1), the most common injury mechanism across the whole sample was supination-plantar flexion (33.6%), followed by supination-external rotation and supination-inversion (each accounting for 25.5%) (table 3). Statistical analysis showed no significant differences, and therefore any correlation, between females and males regarding Dias-Tachdjian mechanisms of injury (table 4).
Although many epidemiological studies have been published on paediatric physeal fractures of the limbs, few focused specifically on the epidemiological data of ankle physeal fractures [8, 9, 13, 16–21]. Our study provided detailed demographic and radiological data, including patterns of injuries, for a large series of children with ankle physeal fractures over a 19-year period.
Our results showed more injuries among males, with more than half of the fractures related to sports injuries. Males were most often injured playing soccer or skateboarding, whereas females were practising gymnastics and horse riding. These observations support the conclusions of previous studies, which showed that soccer, football, basketball, athletics and skateboarding were the most common sports associated with paediatric ankle fractures [6, 16]. After sports, the most frequent causes of injuries were low-energy falls among females and road traffic accidents among males, not only as pedestrians or bicycle riders but also as scooter riders and quadbike drivers. These sex differences are often linked to the male preference for contact sports and for driving vehicles, together with a temperament more prone to risk taking [5, 6, 16, 22–24]. Some authors have stated that this epidemiological distribution could change due to the increasing participation of females in soccer and other contact sports [16]. Despite decades since those historical cohorts, we still found distinct male and female sports preferences instead of the expected overlap in contact sports. We also found more road injuries among males. In some countries (North America), the peak for road accidents among children older than 14 has also been associated with reaching driving age [16].
Contrary to other typical descriptions of the types of fractures affecting paediatric populations, our study did not detect a bimodal age distribution for physeal ankle fractures, which seemed reasonable since physeal fractures mainly occur during the pubertal peak. Our findings suggested that ankle physeal fractures are most common between the ages of 10 and 15 years, when growth is accelerating, and then growth plates begin to fuse. Our study showed that the peak period for fractures was during the pubertal growth spurt, but this was not synchronous for both sexes, occurring at 14 among males and approximately two years earlier, at 12, among females. This peak period for physeal fractures, during the growth spurt, is likely due to the increased weight, muscular strength and activity levels of older children, leading to higher-energy traumas and a greater frequency of ankle physeal fractures [5, 6]. This unimodal distribution contrasts with the bimodal distribution described for other types of physeal fractures, such as those of the elbow and the metatarsals [6].
Our results also indicated seasonal variations in our cohort’s injuries, and they differed from our expectations. Most traumas occurred in the autumn, followed by spring and winter. This was slightly different from what is generally found in the literature, where it is suggested that the most consistent climatic factor related to paediatric trauma is hours of sunshine, with a higher average number of fractures in the summer – estimated to be 2.5 times higher than in winter [14, 25]. The lower frequency of summer fractures may be explained by children leaving Geneva for holidays, with many thus experiencing fractures outside our referral area and thus not being admitted to our hospital.
From a biomechanical perspective, our study suggested that supination was the most common initial foot position at the time of injury, recorded in 84.6% of ankle fractures. External rotation, plantar flexion and inversion were the primary directions of force applied to these supinated feet, in roughly equivalent proportions. When the foot’s initial position was pronation (14.3%), external rotation and eversion were the main directions of force applied.
Our study also showed a similar distribution of fractures according to the Salter-Harris classification as the literature. Salter-Harris type II fractures predominated in our cohort, followed by types III, IV and I. Similarly, in the literature, Salter-Harris type II fractures were the most common ankle physeal fracture, accounting for 32–40% of fractures, followed by types III (25%), IV (up to 25%), I (3–15%) and V (less than 1%) [13, 16, 26]. In our study, Salter-Harris type II fractures were predominant among males and females, with slightly more among males, whereas Salter-Harris types III and IV involved slightly higher proportions of females. Our results also revealed a surprisingly high proportion of transitional ankle physeal fractures, especially among females.
The present research was a retrospective single-centre study based on patients’ electronic medical records, which enabled detailed, standardised data collection, providing accurate findings. However, the study’s retrospective nature was a limitation, as was the challenge of diagnosing Salter-Harris type V fractures, which often require MRI or are only recognised during follow-up [27]. Another limitation is that the data are based on paediatric patients from an urban environment in an industrialised country. Therefore, our epidemiological data may not be representative and generalisable to children in developing countries or rural areas.
Future prospective studies would benefit from collecting standardised data across multiple centres, thus further enhancing our understanding of the epidemiological and causative relationships between risk factors, other variables and clinical and radiological outcomes. Larger sample sizes would also help clarify the incidence of growth disturbances, which remains poorly defined in the literature.
This study provided an in-depth examination of paediatric ankle physeal fractures, including their epidemiology, fracture patterns and mechanisms of injury. There was a slight predominance of these injuries among males, with sports being the leading cause. Isolated physeal fractures of the distal tibial physis were the most common, followed by bimalleolar and distal fibula physeal fractures. Salter-Harris type II was the most prevalent fracture type, accounting for 51% of physeal fractures, followed by types III and IV. The predominant mechanism of injury was a supination-plantar flexion. Future studies should adopt a prospective multicentre design to include more patients and investigate the epidemiology and causative factors contributing to growth disturbances.
The data that support the findings of this study (de-identified individual participant data underlying the results reported in this article, including demographic, clinical, and radiologic data, extracted in an excel dataset) will be made available by the corresponding author or Pr. Ceroni upon reasonable request. Data will be available beginning for 10 years since the approval of the ethics committee. Researchers who submit a methodologically sound proposal will be granted access to the dataset and ethics committee documents.
This study received no funding.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest related to the content of this manuscript was disclosed.
1. Podeszwa DA, Mubarak SJ. Physeal fractures of the distal tibia and fibula (Salter-Harris Type I, II, III, and IV Fractures). Journal of Pediatric Orthopaedics. 2012;32(SUPPL. 1).
2. Langenskiöld A. Traumatic premature closure of the distal tibial epiphyseal plate. Acta Orthop Scand. 1967;38(4):520–31. doi: https://doi.org/10.3109/17453676708989658
3. Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg. 2013 Apr;21(4):234–44. doi: https://doi.org/10.5435/JAAOS-21-04-234
4. Mizuta T, Benson WM, Foster BK, Paterson DC, Morris LL. Statistical analysis of the incidence of physeal injuries. J Pediatr Orthop. 1987;7(5):518–23. doi: https://doi.org/10.1097/01241398-198709000-00003
5. Peterson CA, Peterson HA. Analysis of the incidence of injuries to the epiphyseal growth plate. J Trauma. 1972 Apr;12(4):275–81. doi: https://doi.org/10.1097/00005373-197204000-00002
6. Peterson HA, Madhok R, Benson JT, Ilstrup DM, Melton LJ 3rd. Physeal fractures: Part 1. epidemiology in Olmsted County, Minnesota, 1979-1988. J Pediatr Orthop. 1994;14(4):423–30. doi: https://doi.org/10.1097/01241398-199407000-00002
7. Ogden JA. Injury to the growth mechanisms of the immature skeleton. Skeletal Radiol. 1981;6(4):237–53. doi: https://doi.org/10.1007/BF00347197
8. Fuchs JR, Gibly RF, Erickson CB, Thomas SM, Hadley Miller N, Payne KA. Analysis of Physeal Fractures from the United States National Trauma Data Bank. Children (Basel). 2022 Jun;9(6):914. doi: https://doi.org/10.3390/children9060914
9. Gibly RF, Georgopoulos G, Carry PM, Miller NH. Lower extremity physeal fractures and post-traumatic surgical deformities; National Trauma Data Bank and institutional cohorts. J Clin Orthop Trauma. 2022 Mar;27:101827. doi: https://doi.org/10.1016/j.jcot.2022.101827
10. Barmada A, Gaynor T, Mubarak SJ. Premature physeal closure following distal tibia physeal fractures: a new radiographic predictor. J Pediatr Orthop. 2003;23(6):733–9. doi: https://doi.org/10.1097/01241398-200311000-00010
11. Blondin E, Stourbe O, Plancq MC, Deroussen F, Gouron R, Klein C. Outcomes of pediatric distal tibial physeal fractures. Orthop Traumatol Surg Res. 2022 Oct;108(6):103199. doi: https://doi.org/10.1016/j.otsr.2022.103199
12. Nenopoulos SP, Papavasiliou VA, Papavasiliou AV. Outcome of physeal and epiphyseal injuries of the distal tibia with intra-articular involvement. J Pediatr Orthop. 2005;25(4):518–22. doi: https://doi.org/10.1097/01.bpo.0000158782.29979.14
13. Rohmiller MT, Gaynor TP, Pawelek J, Mubarak SJ. Salter-Harris I and II fractures of the distal tibia: does mechanism of injury relate to premature physeal closure? J Pediatr Orthop. 2006;26(3):322–8. doi: https://doi.org/10.1097/01.bpo.0000217714.80233.0b
14. Salter RB, Harris WR. Injuries Involving the Epiphyseal Plate. J Bone Joint Surg Am. 1963;45(3):587–622. doi: https://doi.org/10.2106/00004623-196345030-00019
15. Dias LS, Tachdjian MO. Physeal injuries of the ankle in children: classification. Clin Orthop Relat Res. 1978;(136). doi: https://doi.org/10.1097/00003086-197810000-00032
16. Goldberg VM, Aadalen R. Distal tibial epiphyseal injuries: the role of athletics in 53 cases. Am J Sports Med. 1978;6(5):263–8. doi: https://doi.org/10.1177/036354657800600507
17. Landin LA, Danielsson LG. Children’s ankle fractures. Classification and epidemiology. Acta Orthop Scand. 1983 Aug;54(4):634–40. doi: https://doi.org/10.3109/17453678308992902
18. Kärrholm J, Hansson LI, Svensson K. Prediction of growth pattern after ankle fractures in children. J Pediatr Orthop. 1983 Jul;3(3):319–25. doi: https://doi.org/10.1097/01241398-198307000-00009
19. Spiegel PG, Cooperman DR, Laros GS. Epiphyseal fractures of the distal ends of the tibia and fibula. A retrospective study of two hundred and thirty-seven cases in children. J Bone Joint Surg Am. 1978 Dec;60(8):1046–50. doi: https://doi.org/10.2106/00004623-197860080-00004
20. Cottalorda J, Béranger V, Louahem D, Camilleri JP, Launay F, Diméglio A, et al. Salter-Harris Type III and IV medial malleolar fractures: growth arrest: is it a fate? A retrospective study of 48 cases with open reduction. J Pediatr Orthop. 2008 Sep;28(6):652–5. doi: https://doi.org/10.1097/BPO.0b013e318182f74c
21. Russo F, Moor MA, Mubarak SJ, Pennock AT. Salter-Harris II fractures of the distal tibia: does surgical management reduce the risk of premature physeal closure? J Pediatr Orthop. 2013;33(5):524–9. doi: https://doi.org/10.1097/BPO.0b013e3182880279
22. Fong DT, Man CY, Yung PS, Cheung SY, Chan KM. Sport-related ankle injuries attending an accident and emergency department. Injury. 2008 Oct;39(10):1222–7. doi: https://doi.org/10.1016/j.injury.2008.02.032
23. D’Angelo F, Solarino G, Tanas D, Zani A, Cherubino P, Moretti B. Outcome of distal tibia physeal fractures: a review of cases as related to risk factors. Injury. 2017 Oct;48 Suppl 3:S7–11. doi: https://doi.org/10.1016/S0020-1383(17)30650-2
24. Steiger C, De Marco G, Cuérel C, Tabard-Fougère A, Chargui M, Dayer R, et al. A retrospective epidemiological cohort study of ankle fractures in children and teenagers. J Child Orthop. 2023 Jun;17(4):348–53. doi: https://doi.org/10.1177/18632521231182424
25. Jung HS, Park MS, Lee KM, Choi KJ, Choi WY, Sung KH. Growth arrest and its risk factors after physeal fracture of the distal tibia in children and adolescents. Injury. 2021 Apr;52(4):844–8. doi: https://doi.org/10.1016/j.injury.2021.01.014
26. Tartaglione JP, Rosenbaum AJ, Abousayed M, DiPreta JA. Classifications in Brief: Lauge-Hansen Classification of Ankle Fractures. Clin Orthop Relat Res. 2015 Oct;473(10):3323–8. doi: https://doi.org/10.1007/s11999-015-4306-x
27. Sferopoulos NK. Bone bruising of the distal forearm and wrist in children. Injury. 2009 Jun;40(6):631–7. doi: https://doi.org/10.1016/j.injury.2009.01.104
The appendix is available in the pdf version of the article at https://doi.org/10.57187/s.4265.