Sex distribution in tuberculosis disease in children, adolescents, and adults in a
low-incidence country: a retrospective population-based cohort study
DOI: https://doi.org/https://doi.org/10.57187/s.4187
Daniela Neudeckera,
Ekkehardt Altpeterb,
Nicole Ritzacd*,
Nora Fritschiae*
a Mycobacterial
and Migrant Health Research Group, University of Basel Children’s Hospital
Basel and Department of Clinical Research, University of Basel, Basel,
Switzerland
b Swiss Federal Office of Public Health, Bern, Switzerland
c Paediatric Infectious Diseases Unit, Children’s Hospital, Lucerne
Cantonal Hospital, Lucerne, Switzerland
d Department of Paediatrics, The Royal Children’s Hospital Melbourne, The
University of Melbourne, Parkville, Australia
e University Children’s Hospital Basel, Basel, Switzerland
* Equal contribution as last authors
Summary
AIM: Globally, tuberculosis
incidence shows notable sex disparity, with higher rates observed in males. While
this pattern is well documented in adults from high-incidence countries, the influence
of sex on tuberculosis incidence in children and adolescents, particularly in low-incidence
settings, remains unclear. This study investigated sex-specific tuberculosis incidence
rates across all age groups, focusing on adolescents, in a low-incidence country.
METHODS: In this retrospective cohort study, data from the
Swiss Federal Office of Public Health (FOPH) tuberculosis database, which centrally
consolidates mandatory notifications from physicians and laboratories across Switzerland,
were analysed from 2000 to 2021. Tuberculosis incidence rates and male-to-female
ratios were calculated and stratified by sex and age. Adolescence was divided into
early (10–14 years) and late (15–19 years) stages for detailed analysis.
RESULTS: Over 22 years, the average tuberculosis incidence in Switzerland
was 6.78 per 100,000 population, with an overall male-to-female ratio of 1:0.75
(p <0.001). Among
the 11,872 notified cases, 832 occurred in adolescents, yielding an incidence rate
of 4.39 per 100,000. In late adolescence, males had a significantly higher
tuberculosis incidence rate (5.73 per 100,000) than females (2.97 per 100,000, p
<0.001), resulting in a male-to-female ratio of 1:0.5. Additionally, data on
asylum seekers revealed nearly twice as many males as females arriving in Switzerland
in late adolescence.
CONCLUSIONS: This study
reveals significant sex disparity in tuberculosis incidence in a country with
low tuberculosis incidence, with males showing higher rates than females beginning
in late adolescence. This discrepancy is likely influenced by the higher influx
of male asylum seekers in adolescence.
Introduction
Sex distribution in tuberculosis exhibits notable
disparities between males and females [1–3],
with male adults accounting for the majority of cases globally. According to the
2023 global tuberculosis report by the World Health Organization (WHO), adult
males represented 55% of cases, while adult females and children accounted for 33%
and 12%, respectively [3]. Several studies
[2, 4, 5] have shown that higher incidence
rates for tuberculosis disease among males are associated with risk factors such
as smoking, alcohol consumption, and exposure to mine-related silicosis, whereas
females are more likely to contract tuberculosis through household contact and HIV
infection [1]. Even in studies
controlling for these risk factors [2, 5],
males show significantly higher odds of developing tuberculosis disease, suggesting
that biological factors [2, 5], particularly
sex hormones, play a crucial role in modulating the immune response to
tuberculosis infection [1, 6, 7]. This biological
influence is further evidenced by the considerable increase in tuberculosis incidence
rates during adolescence [8, 9], coinciding
with hormonal changes.
Despite the well-documented sex differences
in tuberculosis incidence among adults and in high-incidence countries, data are
limited in adolescents, particularly in countries with low tuberculosis incidence,
such as Switzerland. In such countries, tuberculosis epidemiology is heavily influenced
by migration, with most tuberculosis cases occurring among foreign-born individuals,
particularly asylum seekers from tuberculosis-endemic regions [10]. Although women
comprise 50% of asylum seekers
globally, they accounted for only 31% of asylum seekers in Europe from 2008 to 2018
[11]. This disparity underscores the importance
of considering sex, age, and asylum-seeking status when analysing tuberculosis incidence
in low-incidence countries. This study investigated
sex-specific tuberculosis incidence rates in Switzerland – a low-incidence country
– across all age groups, focusing on adolescents. Furthermore, it examined age-related
trends and the impact of migration patterns on observed sex disparities.
Methods
This study was conducted in Switzerland, a
country with a low incidence of tuberculosis, using national surveillance data from
2000 to 2021. The analysis focused on sex-specific tuberculosis incidence rates
across all age groups, with an emphasis on adolescents. Adolescence was categorised
into early adolescence (10–14 years) and late adolescence (15–19 years) [8, 9].
Data were extracted from the mandatory notification
system of the Swiss Federal Office of Public Health (FOPH), which consolidates all
tuberculosis notifications reported by physicians and laboratories. Notifications
are required by Swiss law and include demographic, clinical, and microbiological
data. Physicians report demographic information (e.g. age, sex, and nationality),
clinical presentation (e.g. affected organs), and treatment details (e.g. drugs
used, start dates, and outcomes). Laboratories report microbiological test results,
including microscopy, culture, molecular assays, and drug susceptibility testing.
The Swiss Federal Office of Public Health does
not record information on migration status; therefore, to account for the influence
of migration, additional data on asylum seekers were obtained from the Federal Statistical
Office (FSO). This dataset provided sex and age at arrival for individuals who sought
asylum in Switzerland during the study period.
A tuberculosis case was defined by one of the
following criteria:
- Detection of Mycobacterium tuberculosis
by culture or molecular assays.
- Initiation of treatment with ≥3
antimycobacterial drugs.
The primary outcome was the incidence rate of
tuberculosis stratified by sex and age group. Incidence rates were calculated as
the number of reported cases per 100,000 population per year, using annual population
data from the Federal Statistical Office as the denominator.
Tuberculosis incidence rates and male-to-female
ratios were calculated and compared across age groups using chi-squared (Chi2)
tests. To assess the potential impact of migration, the number of male and female
asylum seekers in Switzerland was analysed. Age at arrival was compared between
sexes using the Mann-Whitney U-test to assess differences in distributions. All
statistical analyses were performed using RStudio (version 2022.07.2) and Excel
(version 2306). Descriptive statistics and graphical visualisations were used to
present the results.
Ethical approval
The Swiss Epidemic Law (EpidA SR 818.101, EpidO
SR 818.101.1, FPHA-ORD SR 818.101.126) provides the legal framework for collecting,
analysing, and reporting notification data in an anonymised format. Ethics clearance
was not required.
Results
Over the 22-year period, 11,872 cases of
tuberculosis were reported in Switzerland, reflecting a mean annual incidence rate
of 6.77 per 100,000 population and an overall
male-to-female ratio of 1:0.75 (Chi2, p <0.001). Among these cases, 832 (7%) were adolescents,
with an overall mean annual incidence rate of 4.39 per 100,000. Adolescent
males had a higher mean annual tuberculosis incidence rate (5.73 per 100,000) than
females (2.97 per 100,000), with a male-to-female ratio of 1:0.5 (Chi2,
p <0.01).
Detailed analysis of tuberculosis incidence
in adolescents in absolute numbers revealed that the increase in incidence began
around the age of 10 years, with an earlier onset in females than in males (figure
1). This rise continued throughout adolescence and into young adulthood, peaking
at age 25 and 30 years in males and females, respectively. Interestingly, in early
adolescence,
females exhibited a higher tuberculosis incidence rate (1.46 per 100,000) than males
(1.15 per 100,000), with a male-to-female ratio of 1:1.2 (Chi2, p = 0.226).
In late adolescence, the tuberculosis incidence rate in males increased to 10.15
per 100,000, significantly higher than that in females (4.44 per 100,000), resulting
in a male-to-female ratio of 1:0.41 (Chi2, p <0.001) (table 1 and
figure 2). In children under 10 years of age, the tuberculosis incidence rate was
low, with no significant sex difference. Notably, the incidence rates in older age
groups (figure 2) may appear exaggerated due to smaller population sizes, making
the rates highly sensitive to small variations in case numbers and potentially leading
to overestimation.

Figure 1Sex distribution in the absolute number of
tuberculosis cases in children, adolescents, and adults per year of age in Switzerland
based on surveillance data from the Swiss Federal Office of Public Health (FOPH)
(2000–2021) and the Federal Statistical Office (FSO) (2010–2021), respectively.
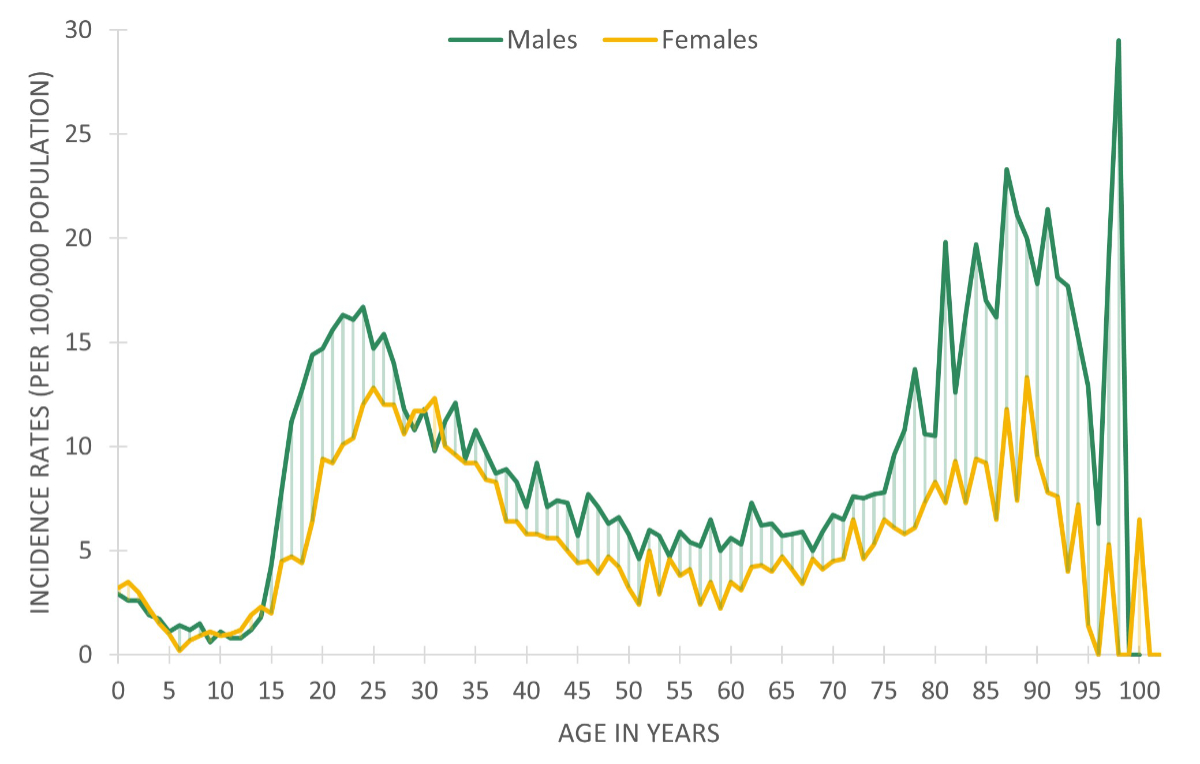
Figure 2Tuberculosis incidence rates by sex and age per 100,000 population in Switzerland.
Table 1Distribution of sex in tuberculosis in the Swiss population, focusing on early and
late adolescence, based on surveillance data (2000–2021) from the Swiss Federal
Office of Public Health (FOPH) and sex distribution in asylum seekers based on surveillance
data (2012–2021) from Federal Statistical Office (FSO).
|
Early adolescence |
Late adolescence |
Adolescence |
All ages |
| 10–14 years |
15–19 years |
10–19 years |
0–100 years |
| M |
F |
M |
F |
M |
F |
M |
F |
| Number of
tuberculosis cases (2000–2021) |
121 |
711 |
832 |
11,872 |
| 55 |
66 |
503 |
208 |
558 |
274 |
6789 |
5083 |
| Male-to-female
ratio of tuberculosis cases |
1:1.2 |
1:0.41 |
1:0.49 |
1:0.75 |
| Chi2,
p = 0.226 |
Chi2,
p <0.001 |
Chi2,
p <0.001 |
Chi2,
p <0.001 |
| Incidence per 100,000 |
1.30 |
7.37 |
4.39 |
6.77 |
| 1.15 |
1.46 |
10.15 |
4.44 |
5.73 |
2.97 |
7.85 |
5.71 |
| Number of asylum
seekers (2010–2021) |
33,998 |
67,290 |
101,288 |
560,575 |
| 18,274 |
15,724 |
48,377 |
18,913 |
66,651 |
34,637 |
348,909 |
211,666 |
| Male-to-female
ratio of asylum seekers |
1:0.86 |
1:0.39 |
1:0.52 |
1:0.61 |
| Chi2,
p <0.001 |
Chi2,
p <0.001 |
Chi2,
p <0.001 |
Chi2,
p <0.001 |
Regarding migration, 560,575 asylum seekers
arrived in Switzerland from 2010 to 2022, of whom 101,288 (18%) were adolescents.
The number of male asylum seekers was nearly twice that of females, with an overall
male-to-female ratio of 1:0.6 (Chi2, p <0.001) and 1:0.5 (Chi2,
p <0.001) for adolescent asylum seekers. More than half of male asylum seekers
arrived between the ages of 15 and 30 years, with a median age at arrival of 25
(IQR 19, 35) years. Female asylum seekers were older upon arrival, with a median
age at arrival of 28 (IQR 19, 39) years (Mann-Whitney U, p <0.001), and approximately
one-third arrived between the ages of 15 to 30 years (table 1 and figure 3).
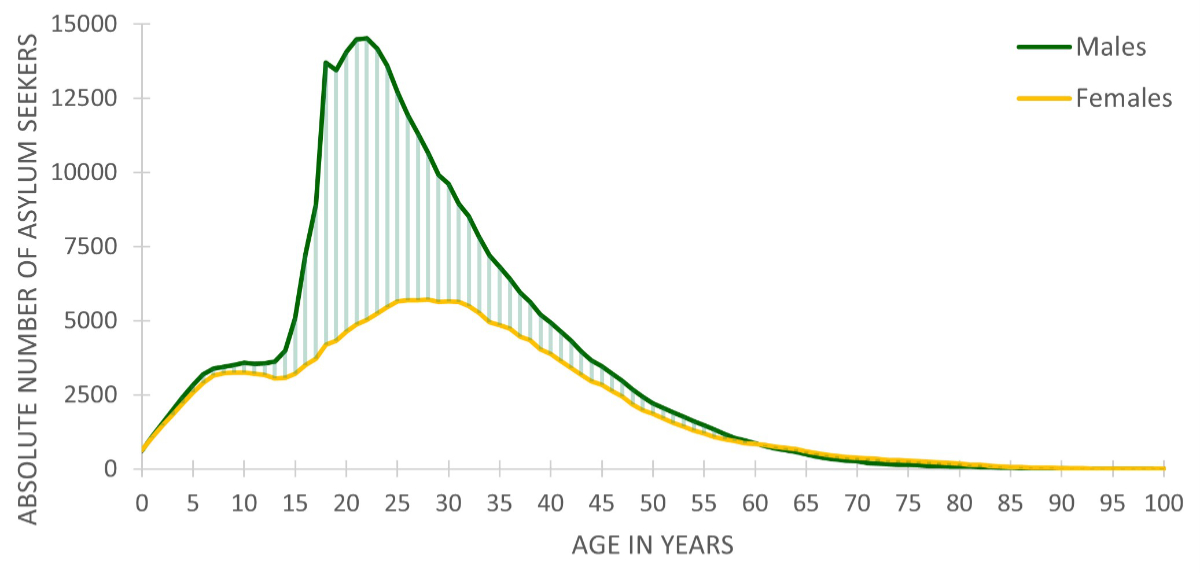
Figure 3Sex distribution in the absolute number of asylum
seekers in children, adolescents, and adults per year of age in Switzerland, based
on surveillance data from the Swiss Federal Office of Public Health (FOPH) (2000–2021)
and the Federal Statistical Office (FSO) (2010–2021), respectively.
Discussion
Our study reveals that the overall annual
tuberculosis incidence in Switzerland is influenced not only by age but also by
sex, particularly during adolescence. In children and early adolescents (under 15
years of age), tuberculosis incidence rates are extremely low and show no significant
sex difference. Although females may exhibit higher incidence rates in early adolescence,
these differences were not significant in our dataset. This observation is consistent
with existing literature suggesting a temporary dominance of tuberculosis incidence
in females during adolescence [12], potentially
due to the earlier onset of puberty in girls compared to boys.
However, in late adolescence, the
tuberculosis incidence rate in males was significantly higher than that in females.
This finding aligns with global reports showing that tuberculosis prevalence is
significantly higher in men than in women. This disparity may be partly attributed
to the biological changes associated with puberty in boys. Moreover, the disproportionate
increase in male asylum seekers in this age group aligns with the higher
tuberculosis incidence observed in adolescent males, suggesting that migration plays
a key role in shaping the sex distribution of tuberculosis cases in Switzerland
[13].
These findings should be interpreted with
caution. Although our study benefits from 22 years of national surveillance data,
several limitations must be considered. Because data on asylum-seeking status
are not included in the mandatory tuberculosis notification system, we were
unable to adjust male-to-female ratios for asylum-seeking status across age groups,
which represents a key limitation. Additionally, individual risk factors such as
comorbidities, prior tuberculosis exposure, and health-seeking behaviour may contribute
to the observed sex disparities. These potential confounders are not recorded in
the national tuberculosis surveillance data; therefore, we could not assess
them. Moreover, there is a mismatch in the timeframes of the available datasets:
national tuberculosis notification data are available from 2000 to 2021, while asylum
seeker data are available from 2010 to 2021. This discrepancy may introduce bias,
leading to over- or underestimation of the influence of migration on male-to-female
tuberculosis incidence ratios.
The generalisability of our findings is limited
to Switzerland and other low-incidence countries with similar healthcare systems
and migration patterns. The observed male predominance in tuberculosis incidence,
particularly in late adolescence, is consistent with findings from a pooled analysis
including data from Europe, the Americas, and Australia, suggesting that biological
and behavioural risk factors contribute beyond high-incidence settings [14].
Our findings provide important epidemiological
insights into the sex distribution of tuberculosis in Switzerland, particularly
among adolescents. This knowledge is valuable for informing public health strategies
and may help clinicians improve tuberculosis diagnosis, especially in adolescents.
Future research incorporating individual-level risk factors, social influences,
and longitudinal follow-up would provide a more comprehensive understanding of sex-specific
tuberculosis disparities, particularly in children and adolescents.
Data sharing statement
Due to the stringent data protection and privacy
terms outlined by the Swiss Federal Office of Public Health, the study data are
not available for open sharing. The data provided by the Swiss Federal Office
of Public Health was anonymised and aggregated, with strict regulations on its use
to prevent any identification of individuals. Therefore, while the analysis is based
on the Swiss Federal Office of Public Health data, sharing the raw data is not permissible
under the data use agreement.
Acknowledgments
Author contributions: Conceptualisation, DN; supervision,
NF; data analysis was conducted by DN and EA; writing original draft, DN, NF, and
NR. All authors revised the manuscript and approved the final draft.
Prof. Nicole Ritz,
MD, PhD
University Children’s
Hospital Basel UKBB
Spitalstrasse 33
CH-4031 Basel
nicole.ritz[at]unibas.ch
References
1. Nhamoyebonde S, Leslie A. Biological differences between the sexes and susceptibility
to tuberculosis. J Infect Dis. 2014 Jul;209 Suppl 3:S100–6. doi: https://doi.org/10.1093/infdis/jiu147
2. Horton KC, Sumner T, Houben RM, Corbett EL, White RG. A Bayesian Approach to Understanding
Sex Differences in Tuberculosis Disease Burden. Am J Epidemiol. 2018 Nov;187(11):2431–8.
doi: https://doi.org/10.1093/aje/kwy131
3. Global tuberculosis report 2023. Geneva: World Health Organization. Available from:
https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2023
4. Horton KC, MacPherson P, Houben RM, White RG, Corbett EL. Sex Differences in Tuberculosis
Burden and Notifications in Low- and Middle-Income Countries: A Systematic Review
and Meta-analysis. PLoS Med. 2016 Sep;13(9):e1002119. doi: https://doi.org/10.1371/journal.pmed.1002119
5. Nguyen HV, Brals D, Tiemersma E, Gasior R, Nguyen NV, Nguyen HB, et al. Influence
of Sex and Sex-Based Disparities on Prevalent Tuberculosis, Vietnam, 2017-2018. Emerg
Infect Dis. 2023 May;29(5):967–76. doi: https://doi.org/10.3201/eid2905.221476
6. Neyrolles O, Quintana-Murci L. Sexual inequality in tuberculosis. PLoS Med. 2009 Dec;6(12):e1000199.
doi: https://doi.org/10.1371/journal.pmed.1000199
7. Zhao Y, Ying H, Demei J, Xie J. Tuberculosis and sexual inequality: the role of sex
hormones in immunity. Crit Rev Eukaryot Gene Expr. 2012;22(3):233–41. doi: https://doi.org/10.1615/CritRevEukarGeneExpr.v22.i3.60
8. Snow KJ, Cruz AT, Seddon JA, Ferrand RA, Chiang SS, Hughes JA, et al. Adolescent tuberculosis.
Lancet Child Adolesc Health. 2020 Jan;4(1):68–79. doi: https://doi.org/10.1016/S2352-4642(19)30337-2
9. Snow KJ, Sismanidis C, Denholm J, Sawyer SM, Graham SM. The incidence of tuberculosis
among adolescents and young adults: a global estimate. Eur Respir J. 2018 Feb;51(2):1702352.
doi: https://doi.org/10.1183/13993003.02352-2017
10. Lönnroth K, Mor Z, Erkens C, Bruchfeld J, Nathavitharana RR, van der Werf MJ, et al. Tuberculosis
in migrants in low-incidence countries: epidemiology and intervention entry points.
Int J Tuberc Lung Dis. 2017 Jun;21(6):624–37. doi: https://doi.org/10.5588/ijtld.16.0845
11. Schiele M. The Role of Gender in Asylum Migration to Europe: Analyzing Country-Level
Factors of Gendered Selection of Asylum Seekers to Europe. J Immigr Refug Stud. 2024:1–16.
10.1080/15562948.2023.2298515
12. Thakur S, Chauhan V, Kumar R, Beri G. Adolescent Females are More Susceptible than
Males for Tuberculosis. J Glob Infect Dis. 2021 Jan;13(1):3–6. doi: https://doi.org/10.4103/jgid.jgid_229_20
13. Fritschi N, Schmidt AJ, Hammer J, Ritz N; Swiss pediatric surveillance unit. Pediatric
Tuberculosis Disease during Years of High Refugee Arrivals: A 6-Year National Prospective
Surveillance Study. Respiration. 2021;100(11):1050–9. doi: https://doi.org/10.1159/000517029
14. Peer V, Schwartz N, Green MS. Corrigendum: gender differences in tuberculosis incidence
rates-A pooled analysis of data from seven high-income countries by age group and
time period. Front Public Health. 2023 Feb;11:1157235. doi: https://doi.org/10.3389/fpubh.2023.1157235