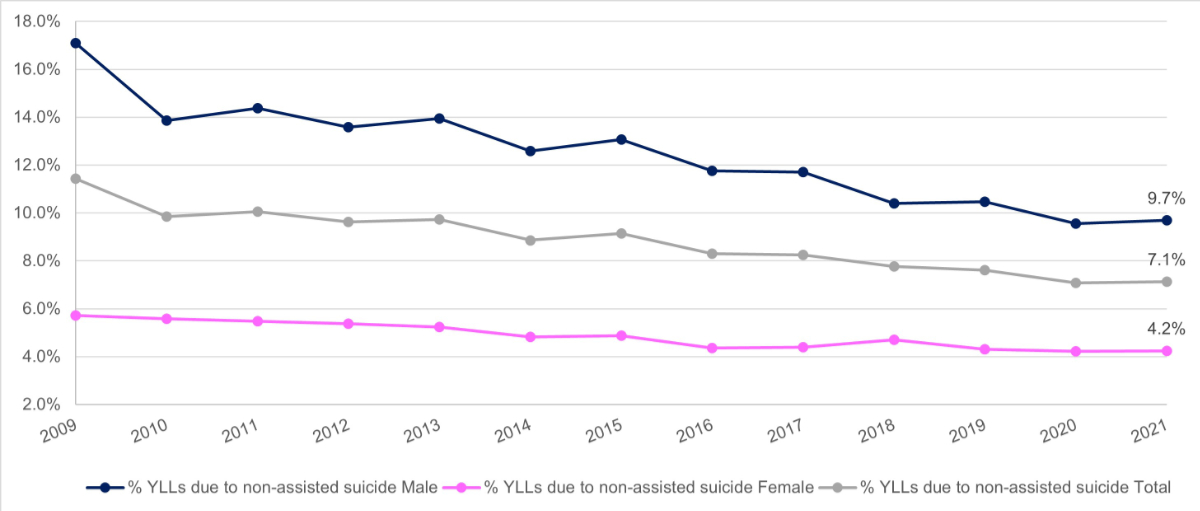
Figure 1Trend in the percentage of total years of life lost (YLLs) which are attributable to suicide in Switzerland from 2009 to 2021 for males, females and total suicide.
DOI: https://doi.org/10.57187/s.3522
disability-adjusted life-years
years lived with disability
years of life lost
Globally, suicide is a leading cause of death in people aged 15–29 [1]. The European average suicide rate was 12.9 per 100,000 in 2019 [2]. Lithuania and Russia had the highest national rates (26.1 and 25.1 per 100,000 respectively) and Turkey had the lowest rate at 2.6 suicides per 100,000. Switzerland ranked 16th (14.5 per 100,000) among the 41 countries studied, and surrounding countries Austria, France and Germany had similar rates [2]. The Federal Statistical Office and the Swiss Health Observatory recorded 994 non-assisted suicides and reported an estimated rate of 11.6 per 100,000 in 2021 [3].
The Lancet reported that in 2021 the age-standardised rate of self-harm was 9.0 per 100,000 (8.3 to 9.6) [19]. The same study noted self-harm as the tenth leading cause of death in high-income countries (10.8 per 100,000) [19]. Self-harm is, in this capacity, the only available indicator for suicidality. Suicidality is defined in this article as all suicidal behaviours including suicidal thoughts, self-harm, attempted suicide and suicide. The increasing severity of risk behaviour and outcome are not reflected in this umbrella term.
Switzerland is one of the few countries where assisted suicide is legally permitted under specific conditions. However, this study specifically excludes assisted suicides from its analysis, focusing instead on non-assisted suicides and attempted suicides, which continue to pose significant public health challenges. These challenges include but are not limited to: providing mental healthcare, destigmatising mental health, preventing suicide and identifying risk factors.
On the basis of a bulletin published by the Federal Statistical Office in 2019, the attempted suicide rate in 2017 was 467 per 100,000, translating to roughly 33,000 (±11,000) attempted suicides per year in the Swiss population aged 15+ [4]. It is important to note that this data excludes assisted suicide as well as people in psychiatric care, prisons or seeking asylum – thereby neglecting relevant subgroups of the population known to exhibit suicide-related behaviours.
Establishing the veracity of suicide and attempted suicide numbers is difficult, both in Switzerland and beyond. This is likely related to the absence of strong data, which stems from the lack of reporting infrastructures, and common international definitions, indicators and guidelines [5]. In the past decade, Switzerland has committed to improving mental healthcare. In 2014, a motion to strengthen suicide prevention at the national level was adopted by the Council of States. The Federal Office of Public Health (FOPH) was mandated to present and implement an action plan for suicide prevention [6].
The aim of the present analysis was to estimate the burden of disease for non-assisted suicide and attempted suicides in Switzerland; to analyse patterns by sex and age group; and to relate the burden of disease to the overall national in Switzerland.
The burden of disease is described by indicators reflecting cause-specific death and disability and presented as disability-adjusted life-years (DALYs). The analysis excluded assisted suicides. Suicide- and attempted suicide-specific DALYs were calculated by adding the sum of years of life lost (YLL) due to deaths by suicide and years lived with disability (YLD), which describes the years lived with a disability relating specifically to non-fatal attempted suicides.
(1)
YLLs due to suicide were calculated by subtracting average age at death (AAD) from standard life expectancy (LE) then multiplying the result by the total number of cause-specific deaths (n). In this case it was the number of non-assisted suicides registered by the Federal Statistical Office:
(2)
Mortality and life expectancy data collected for the YLL estimation was obtained from the Federal Statistical Office in November 2022 [7]. This data is routinely collected by healthcare providers and compiled on an annual basis. Additional data collected from the Federal Statistical Office included non-assisted suicide rates stratified by sex, age group, method of suicide and location. The YLLs were calculated and compared with YLL estimates for all-cause mortality and ischaemic heart disease for the period from 2009 to 2021. At the time of the analysis, Federal Statistical Office data was available up to 2021. The year 2009 was selected as the starting point, since this was the first year that the Federal Statistical Office began distinguishing between data for assisted and non-assisted suicide.
The data selected for the YLL calculations included people who lived in Switzerland, died and whose deaths were reported to the Federal Statistical Office. Life expectancy for the Swiss population was obtained from the Federal Statistical Office database and applied without adjustment. Average age at death was established by subtracting LE from the median age of the age group with the highest incidence of non-assisted suicide (50–59). The sex disparity in average age at death is a result of the shifting trends in other age groups [(40–49) and (60–69)].
YLDs as defined within the scope of this analysis refers exclusively to the suicide attempt and its direct consequences, not to any underlying mental health problems that could lead to or stem from an attempted suicide. YLDs were obtained by multiplying disease incidence (I) with disability weights (DW) and average duration to remission or death (AD).
(3)
Data sources collected for the YLD estimation included peer-reviewed articles on measuring the burden of disease and estimating disability weights related to non-assisted suicide [8, 9]. Case fatality ratios for each method and the duration of disability related to surviving an attempted suicide were estimated and results from a multicentre study on suicidal behaviour in Switzerland used as supplementary information [14].
The reference value for attempted suicide incidence (33,000) was derived from Peter and Tuch’s publication [4] which presented an estimated range of 23,000–42,000 suicide attempts per year. A sex distribution of suicide attempts (80% female to 20% male) was applied for the calculation of the YLDs. The WHO/MONSUE Multicentre Study on Suicidal Behavior [10] noted various methods and respective sex distributions of each suicide attempt method. Reference, minimum and maximum incidences for each suicide attempt method according to Steffen et al. [10] were calculated and stratified based on the proposed sex proportions. For each method, case fatalitydata, approximations of survivor health outcomes and recovery prognoses were used to define appropriate reference values for disability weight and average duration to remission or death (table 1). DALY calculations were done per year. Thus, the maximum duration of disability for the average duration to remission or death variable was capped at one year.
Table 1Estimated disability of attempted suicide method in Switzerland, sex distribution*, assigned disability weights and average duration to remission or death.
| Method of suicide attempt* | Proportion of suicide attempt method by sex* | Disability weight (0–1) | Average duration to remission or death (years) | |||||
| Male | Female | Reference | Minimum | Maximum | Reference | Minimum | Maximum | |
| Drug intoxication | 43.7% | 72.8% | 0.2 | 0.1 | 0.3 | 0.2 | 0.05 | 0.4 |
| Poisoning | 1.9% | 2.6% | 0.2 | 0.1 | 0.3 | 0.25 | 0.05 | 0.45 |
| Hanging | 8.9% | 1.0% | 0.6 | 0.5 | 0.7 | 0.5 | 0.3 | 0.7 |
| Firearm | 3.3% | 0.1% | 0.5 | 0.4 | 0.6 | 1 | 0.8 | 1.2 |
| Jumping | 10.5% | 7.4% | 0.4 | 0.3 | 0.5 | 0.5 | 0.3 | 0.7 |
| Train | 4.1% | 1.7% | 0.5 | 0.4 | 0.6 | 1 | 0.8 | 1.2 |
| Cutting | 22.6% | 10.1% | 0.05 | 0.01 | 0.15 | 0.2 | 0.05 | 0.4 |
| Alcohol | 1.2% | 2.3% | 0.1 | 0.01 | 0.2 | 0.1 | 0.05 | 0.3 |
| Other | 3.8% | 2.0% | 0.1 | 0.01 | 0.2 | 0.2 | 0.05 | 0.4 |
* Methods and proportion of suicide attempts by sex proposed by Steffen et al. (2011) [10].
A sensitivity analysis was conducted separately for the variables thought to most strongly influence YLD results: attempted suicide incidence by method, disability weight, average duration to remission or death and sex distribution of attempted suicide methods. This was necessary to account for the uncertainty regarding the assigned reference values and provided the main estimate with which to work.
This study involved secondary analysis of anonymised, publicly available data. No new data was collected, and no direct interaction with study participants occurred. Consequently, no informed consent was required, and no ethics review was necessary.
No study protocol was registered for this secondary data analysis as it involved the use of pre-existing, publicly available data.
The collection of pre-existing data made it possible to calculate an estimated burden of disease for suicide and attempted suicide in Switzerland. The calculations described in the methodology resulted in an estimated 33,410 DALYs attributable to non-assisted suicide and attempted suicide in Switzerland. For the year 2021, these DALYs comprised 31,155 YLLs and 2255 YLDs. Table 2 provides an overview of the Federal Statistical Office data and results used to calculate the burden of non-assisted suicide in Switzerland.
Table 2Estimated burden of non-assisted suicide in Switzerland for 2021, calculated from the Federal Statistical Office mortality statistics.
| Male | Female | Average/total | |
| Average life expectancy [at birth]* | 81.6 | 85.7 | 83.7 |
| Total deaths** | 35,095 | 36,071 | 71,166 |
| Average age at death [all-cause]*** | 75 | 80 | 77 |
| Years of life lost (YLL) [all-cause]*** | 231,627 | 205,605 | 437,232 |
| Suicides** | 710 | 284 | 994 |
| Average age at death*** | 50 | 55 | 53 |
| Years of life lost (YLL) [suicide]*** | 22,436 | 8719 | 31,155 |
| Years lived with disability (YLD) [attempted suicide]**** | 701 | 1554 | 2255 |
| Disability-adjusted life-years (DALYs) | 23,137 | 10,273 | 33,410 |
| % deaths attributable to suicide*** | 2% | 0.8% | 1.4% |
| % years of life lost attributable to suicide*** | 9.7% | 4.2% | 7.1% |
* Source: Federal Statistical Office – Indicators of mortality in Switzerland, 1970–2021.
** Source: Federal Statistical Office – Major causes of death, by age, female and male.
*** Source: Extrapolation from dataset; see Methods section.
**** Source: Reference incidence of the modelled estimation of years lived with disability (YLDs) for attempted suicide; see table 3.
Overall, non-assisted suicides accounted for 1.4% of all deaths in Switzerland in 2021. In terms of YLLs however, suicide contributes 6.4% to annual years of life lost. This is a significant decrease from the 11.4% contribution reported for the year 2009.
This data also revealed a stark sex gap: male suicides account for 2% of all deaths, whereas female suicides account for 0.8% of deaths. The sex discrepancy trend also applies to the observed YLL proportions: of the 31,155 YLLs attributable to non-assisted suicide in Switzerland in 2021, the male contribution was higher than the female contribution by a factor of 2.6.
Figure 1Trend in the percentage of total years of life lost (YLLs) which are attributable to suicide in Switzerland from 2009 to 2021 for males, females and total suicide.
The estimated years lived with disability in Switzerland associated with attempted suicide was determined to be 2255 YLDs with a total range of 552 to 6557 YLDs. In the reference case, males and females accounted for 701 and 1554 YLDs, respectively. Table 3 provides the reference values, uncertainty ranges and results of the YLD estimation.
Table 3Modelled estimation of years lived with disability by method and sex for attempted suicide in Switzerland using the incidence estimate and method distribution proposed by Steffen et al. (2011) [10].
| Attempted suicide years lived with disability, sex distribution (80% female: 20% male) | ||||
| Reference incidence | Minimum incidence | Maximum incidence | ||
| Male | Drug intox | 115 | 10 | 440 |
| Poisoning | 6 | 0 | 22 | |
| Hanging | 176 | 61 | 366 | |
| Firearm | 109 | 49 | 200 | |
| Jumping | 139 | 43 | 309 | |
| Train | 135 | 60 | 248 | |
| Cutting | 15 | 1 | 114 | |
| Alcohol | 1 | 0 | 6 | |
| Other | 5 | 0 | 26 | |
| Subtotal | 701 | 225 | 1730 | |
| Female | Drug intox | 769 | 67 | 2935 |
| Poisoning | 34 | 2 | 118 | |
| Hanging | 79 | 28 | 165 | |
| Firearm | 13 | 6 | 24 | |
| Jumping | 391 | 123 | 870 | |
| Train | 224 | 100 | 411 | |
| Cutting | 27 | 1 | 204 | |
| Alcohol | 6 | 0 | 46 | |
| Other | 11 | 0 | 54 | |
| Subtotal | 1554 | 327 | 4827 | |
| Total | 2255 | 552 | 6557 | |
Given the uncertainties regarding the true incidence of attempted suicides in Switzerland, the sensitivity analysis estimates the YLD to be in the range of 552 (23,000 attempts) to 6557 (42,000 attempts). Further, the analysis of the uncertainty of the reference values found that incidence and sex distribution of attempted suicide were the most impactful factors, while disability weights and average duration to remission or death had little impact on the variation in YLD estimates. Thus, the incidence of attempted suicide and related sex distribution are significantly more relevant to the precision of the YLD estimate than are the disability weight and average duration to remission or death. The present study found that in 2021, 31,155 YLLs and 2255 YLDs stemmed from suicide-related mortality and morbidity. The result is an estimate of 33,410 DALYs attributable to non-assisted suicide and attempted suicide.
The Swiss Health Observatory describes major causes of loss of potential life-years. Excluding the “all other” category (21.3%), only cancers (21.7%) and cardiovascular diseases (13.1%) cause more years of life lost (YLLs) than suicide (9.6%) [11]. Of the cardiovascular diseases, ischaemic heart disease is the most prevalent cause of mortality in Switzerland. In 2021 there were 6227 deaths due to ischaemic heart disease [7]. Based on the data provided in table 2, this equates to roughly 41,721 YLLs. While there were six times as many ischaemic heart disease deaths (n = 6227) as non-assisted suicides (n = 994) in 2021, the difference in terms of YLLs is substantially lower: 41,721 YLLs due to ischaemic heart disease versus 30,516 YLLs due to non-assisted suicide.
A likely explanation for this is the affected age group. Non-assisted suicide is the leading cause of death in people under 50 in Switzerland [12]. In 2019, in the age group 15–44, 24% of deaths among males and 16% of deaths among females were due to non-assisted suicide. Looking further into this age demographic revealed that 30% of deaths in people aged 20–24 were due to non-assisted suicide, and an additional 9% of deaths were due to substance use disorders. This does not discount the fact that the suicide rates increase with age. However, the age factor does explain the contribution to YLLs. The younger the death, the greater the loss of potential life years. Obsan reports that raw suicide rates (per 100,000) in Switzerland (5-year average, 2017–2021) were 8.7 for the age group 15–34, while the rate was 27.5 for the age group 80+.
The evaluated time span, 2009 to 2021, saw a decline in the burden of disease of non-assisted suicide, most importantly among male YLLs. Overall, a declining trend has been observed both in the absolute numbers of non-assisted suicide and in the loss of potential life years [11]. Considering population growth, increasing life expectancy and the ageing demographic pyramid – the magnitude of this reduction is substantial. Furthermore, data from 2020 and 2021 indicate that the Covid-19 pandemic did not negatively impact the burden of disease attributable to suicide [13]. Compared to previous years, the decrease in non-assisted suicides was comparatively large. That being said, the mental health effects of the pandemic on the Swiss population may differ from the observed non-assisted suicide rate. Werdin and Wyss (2024) found that while challenges in mental healthcare provision were exacerbated by the pandemic, it has simultaneously drawn the attention of policymakers to the importance of suicide prevention and improved mental healthcare [20]. It is important to note here that while the burden of years lived with disability (YLDs) due to attempted suicide is substantial, YLLs vastly outweigh YLDs in their contribution to the burden of disease of non-assisted suicide and attempted suicide in Switzerland. Of the 33,410 disability-adjusted life-years (DALYs) attributable to suicide and attempted suicide in 2021, 31,155 units are YLLs while 2255 are YLDs. When assessing this difference, the male-specific DALYs (n = 23,137) reveal a staggering 32:1 ratio (22,436 YLL: 701 YLD).
The sensitivity analysis revealed that incidence and sex distribution of attempted suicides were the most impactful factors in determining YLDs. To determine the incidence of each suicide attempt method, it was essential to know the approximate sex ratio of attempted suicide overall, to correctly estimate both method-specific incidences and sex-specific YLDs. The data clearly showed that males die by suicide more frequently than females. However, according to Muheim et al. [14], females predominantly attempt suicide while males generally complete their suicide attempts. Similarly, a Polish study found that 80% of attempted suicides were by females and 20% by males [15]. This tendency was corroborated by Keller-Guglielmetti and Walter [16] who found that females preferred soft suicide methods such as drug intoxication that were often less effective, while males tended to choose asphyxiation and firearms as suicide methods, which are significantly more effective. This sex gap in suicidality remains a distinct element in the epidemiology and burden of non-assisted suicide in Switzerland.
Regardless of age or sex, it is clear that non-assisted suicide and attempted suicides are a significant contributor to the burden of disease in Switzerland. The risk is that if left untreated, the mental health crisis will lead to increasing loss of life and potential. In December 2022, Spectra published an article on the progress of the aforementioned action plan [17, 18]. The authors found that substantial progress has been made in the promotion of mental health in general, specifically when it comes to strengthening resources, support services, and increasing awareness of suicidality. That said, there is still more to be done. Objectives that have yet to be achieved include reducing access to means and methods of suicide, improving aftercare offers for surviving relatives of suicide victims and enhancing research and data [17].
The findings presented in this study provide information that has important implications for novel potential policy measures. Non-assisted suicides and attempted suicides may be preventable, and suspected cases of mental health distress should be addressed by healthcare providers. Enhancing surveillance methods and training healthcare providers and first responders to identify at-risk patients should be a priority. To evaluate the relevance for public health and the need for improved measures aimed at preventing non-assisted suicide, a comprehensive and sustainable reporting system should be established. This could enable enhanced identification of attempted suicides and provide reliable long-term data for evidence-based decision-making.
This secondary data analysis has certain limitations in the methodology and analysis of the data. The variable life expectancy at birth was used for the DALY calculations, although people do not die by suicide the year they are born. Life expectancy at birth was taken for each year, which skews the results towards a larger YLL since life expectancy has been trending upwards for decades. In addition, the variable average age at death required a standardised reference value, which was defined as average age at death = 50 for males and average age at death = 55 for females. Although retroactive fitting of life expectancy to average age at death would have increased the specificity of YLL results, this level of complexity was outside the scope of this project. Although detailed information about the age at suicide death was available on the Federal Statistical Office database, a standardised value was required for the YLL calculation. In a more accurate model, individual average age at deaths and retrofitted life expectancy adjusted for year of birth would be used to calculate YLLs for each suicide.
Furthermore, defining disability related to attempted suicides is a complex task for many reasons; psychosocial and physical disability relating to an attempted suicide vary depending on many factors, for example the method used in the attempt, mental health resilience, openness to treatment, severity of injury and strength of support network. In quantifying disability weights associated with attempted suicides, one must exclude psychological or physical diagnoses that may relate to the attempt as this would result in double counting. As specified in the Methods section, only YLDs directly related to the suicide attempt were considered. It could be however that the individual’s experienced disability burden is contingent on additional factors.
Non-assisted suicide and attempted suicide contribute significantly to Switzerland’s national burden of disease with an estimated 6.4% of YLLs in 2021. Unlike in the case of assisted suicide, where the underlying motivations often relate to chronic and untreatable suffering, many catalysts of suicide attempts and non-assisted suicides relate back to treatable causes. In order to prevent non-assisted suicide and attempted suicides, a strong public healthcare system allowing early diagnosis and adequate treatment of mental health disorders is essential.
The study’s findings are particularly relevant in an international context where the legal status and societal attitudes towards suicide, both assisted and non-assisted, vary widely, influencing both the prevalence of suicides and the public health strategies employed to address them. Exploring the burden of non-assisted suicide in Switzerland revealed that the primary contributing factor to DALYs associated with non-assisted suicide and attempted suicides were the YLLs; only a small contribution of YLDs due to attempted suicide was found. The declining trend in non-assisted suicides is therefore a significant development in the reduction of DALYs. The Federal Statistical Office published an article on this declining trend and noted that in 2020, the number of non-assisted suicides in Switzerland fell below 1000 for the first time since 1964 [13]. Establishing appropriate systems to detect, report and prevent non-assisted suicides would further contribute to the reduction of suicides. With the suicide prevention action plan well underway, additional steps towards reducing non-assisted suicide in Switzerland are expected.
AM thanks her master’s thesis supervisors and co-authors Kaspar Wyss and Sarah Rajkumar for their enduring support and insights. The publication of this work would not have been possible without the additional help of the first responders of Basel-Stadt’s Emergency Response and Police Forces whose insight and experiences provided valuable context to the analysed data and reality of non-assisted suicide and attempted suicide in Switzerland.
This publication received no specific funding.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest related to the content of this manuscript was disclosed.
1. WHO. - Suicide Worldwide in 2019: Global Health Estimates. Geneva: World Health Organization; 2021. Available at: https://www.who.int/publications/i/item/9789240026643
2. The Global Economy. Suicides - Country rankings. Available at: https://www.theglobaleconomy.com/rankings/suicides/Europe/
3. Schweizerisches Gesundheitsobservatorium. Suizid und Suizidhilfe. Available at: https://ind.obsan.admin.ch/indicator/obsan/suizid-und-suizidhilfe
4. Peter C, Tuch A. Suizidgedanken und Suizidversuche in der Schweizer Bevölkerung (Obsan Bulletin 7/2019). Neuchâtel: Schweizerisches Gesundheitsobservatorium; 2019., Available at https://www.obsan.admin.ch/sites/default/files/obsan_bulletin_2019-07_d_0.pdf
5. WHO - National Suicide Prevention Strategies. Progress, Examples and Indicators. Geneva: World Health Organization; 2018. Available at: https://www.who.int/publications/i/item/national-suicide-prevention-strategies-progress-examples-and-indicators
6. Walter E, Schmuki MD, Bürli C, Amstad F, Haas A, Schibli D, et al. (2016). Suizidprävention in der Schweiz Ausgangslage, Handlungsbedarf und Aktionsplan. Bundesamt für Gesundheit (BAG). Available at: https://repository.publisso.de/resource/frl:6399838/data
7. Bundesamt für Statistik. Spezifische Todesursachen. Available at: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitszustand/sterblichkeit-todesursachen/spezifische.html
8. Kerkhof A. Calculating the burden of disease of suicide, attempted suicide, and suicide ideation by estimating disability weights. Crisis. 2012 Jan;33(2):63–5. doi: https://doi.org/10.1027/0227-5910/a000161
9. van Spijker BA, van Straten A, Kerkhof AJ, Hoeymans N, Smit F. Disability weights for suicidal thoughts and non-fatal suicide attempts. J Affect Disord. 2011 Nov;134(1-3):341–7. doi: https://doi.org/10.1016/j.jad.2011.05.020
10. Steffen T, Maillart A, Michel K, Reisch T. (2011). Monitoring des suizidalen Verhaltens in der Agglomeration Bern der Jahre 2004 bis 2010. Available at: https://www.npg-rsp.ch/fileadmin/npg-rsp/Themen-Bibliothek/Fachthemen/Reisch_2011_Suizidales_Verhalten_Bern.pdf
11. Schweizerisches Gesundheitsobservatorium. Verlorene Potenzielle Lebensjahre. Available at: https://ind.obsan.admin.ch/indicator/obsan/verlorene-potenzielle-lebensjahre
12. Institute for Health Metrics and Evaluation. GBD Compare – VizHub. Available at: https://vizhub.healthdata.org/gbd-compare/
13. Bundesamt für Statistik. Weniger als 1000 Suizide im Jahr 2020 - Langjährige Tendenz weiter sinkend. Available at: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitszustand/sterblichkeit-todesursachen.assetdetail.23446122.html. Press Release
14. Muheim F, Eichhorn M, Berger P, Czernin S, Stoppe G, Keck M, Riecher-Rössler A. Suicide attempts in the county of Basel: results from the WHO/EURO Multicentre Study on Suicidal Behaviour. Swiss Med Wkly. 2013 May 19;143(1920):w13759. https://doi.org/
15. Tsirigotis K, Gruszczynski W, Tsirigotis M. Gender differentiation in methods of suicide attempts. Med Sci Monit. 2011 Aug;17(8):PH65–70. doi: https://doi.org/10.12659/MSM.881887
16. Keller-Guglielmetti E, Walter E. (2015). Epidemiologie von Suiziden, Suizidversuchen und assistierten Suiziden in der Schweiz. Realisierung im Auftrag des BAG: Amina Trevisan (Doktorandin an der Universität Basel). Available at: https://www.npg-rsp.ch/fileadmin/npg-rsp/Themen-Bibliothek/Fachthemen/BAG_2015_Suizid_Epidemiologie.pdf
17. Spectra. Suizidprävention in der Schweiz macht Fortschritte. Available at: https://www.spectra-online.ch/de/spectra/news/suizidpraevention-in-der-schweiz-macht-fortschritte-1061-29.html
18. Trageser J, Petry C, Reisch DT (2021). Zwischenstand Umsetzung Nationaler Aktionsplan Suizidprävention Schlussbericht. Bundesamt für Gesundheit (BAG). Available at: file:///C:/Users/smw/Downloads/21-09-01_Schlussbericht%20Ist-Analyse_Gesamtdokument_d.pdf
19. Naghavi M, Ong KL, Aali A, Ababneh HS, Abate YH, Abbafati C, et al.; GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024 May;403(10440):2100–32. doi: https://doi.org/10.1016/S0140-6736(24)00367-2
20. Werdin S, Wyss K. Advancing suicide prevention in Germany, Austria and Switzerland: a qualitative study. Front Public Health. 2024 May;12:1378481. doi: https://doi.org/10.3389/fpubh.2024.1378481