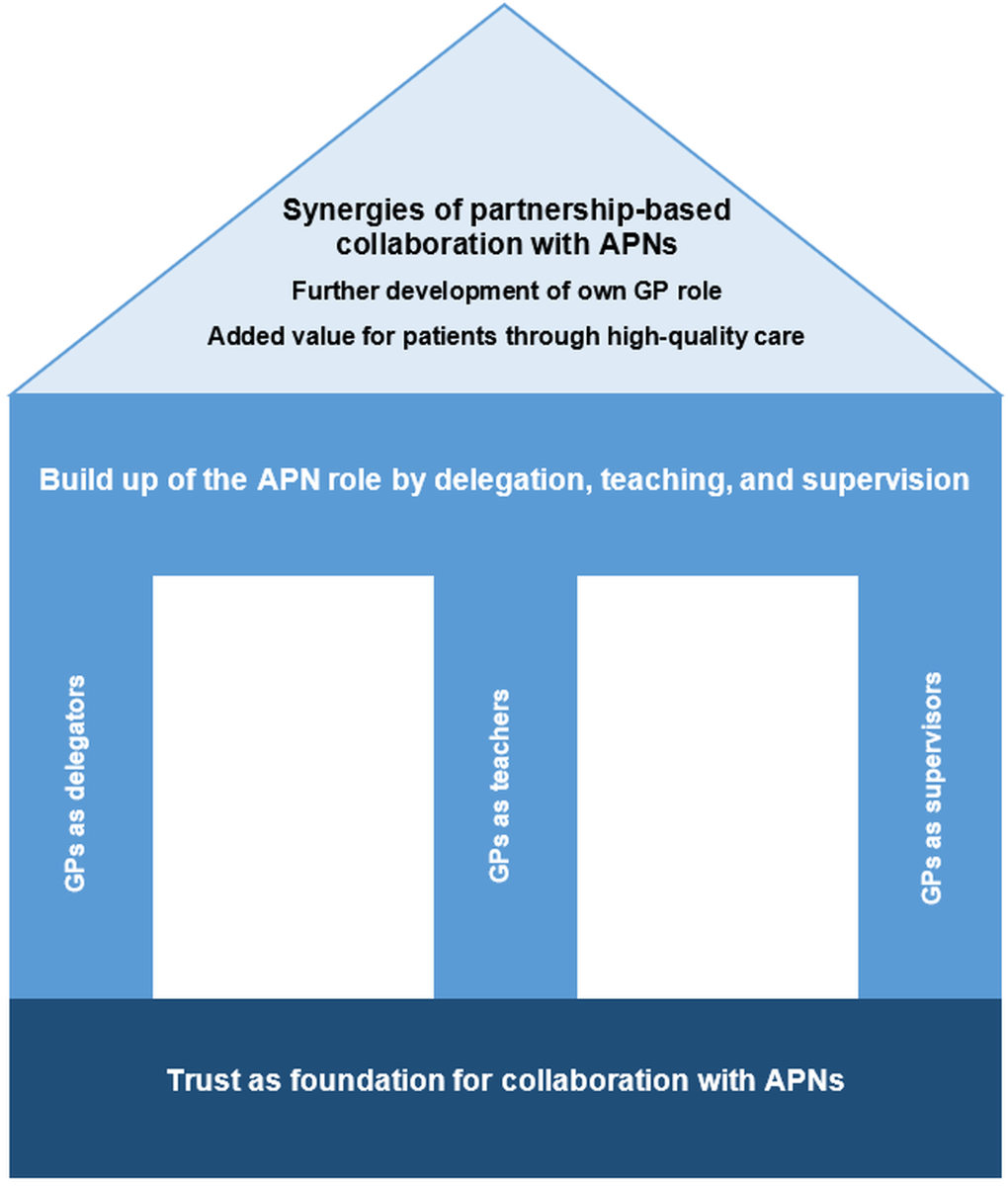
Figure 1 New Care Model: integration of an advanced practice nurse (APN) into general practitioner (GP) primary care.
DOI: https://doi.org/10.4414/SMW.2022.w30199
Accompanying Switzerland’s demographic aging, a high prevalence of chronic illness is exacerbating its shortage of general practitioners (GPs) [1–3]. By 2030, the Swiss Health Observatory [4] estimates that demand for outpatient treatments will exceed supply by 40%.
Managing this shortfall while providing chronically ill and older patients with needed care requires the establishment of new care models. For example, systems that include advanced practice nurses (APNs) with chronic care expertise are already demonstrating collaborative advantages, boosting both quality and efficiency in GP practices [1]. Working alongside GPs, APNs have the medical knowledge, clinical competencies and practical skills to provide evidence-based care suitable for patients with complex care needs. Several international studies have confirmed their effectiveness in this context [5–8].
APN certification requires a master’s degree. The APN designation covers various roles, mainly nurse practitioners and clinical nurse specialists. The many possible mixes produce a continuum of APN roles [9]. Clinical nurse specialists usually work in hospitals as expert clinicians with advanced expertise, for example in caring for patients with complex diseases or conditions. Additionally, they are typically involved in non-clinical activities including education and support for staff nurses. Nurse practitioners often work in outpatient settings, providing direct patient care, providing advanced assessments and treating various conditions or illnesses.
In primary care practices, the APN role is weighted towards the nurse practitioner side, focusing largely on the care of chronically ill patients in medical practices, patients’ homes or nursing homes, including house calls or rounds in nursing homes, performing clinical assessments, ordering diagnostic tests, prescribing medications (under GPs’ supervision) and following up on treatment plans. They focus on comprehensive, patient-centred care of patients and their families, including the promotion of self-management, health prevention and advance care planning (table 1).
The development and implementation of new roles such as those filled by APNs depend on numerous factors, e.g., the clarification of responsibilities and the reorganization of tasks. Similar issues emerge during their introduction into primary care internationally. In all cases, though, their integration demands that existing models be rearranged. This can lead to resistance among GPs [10, 11]. Furthermore, in Switzerland, which is still in the early stages of developing APN roles in primary care, few pioneer models have been established so far. This shortage can lead to confusion regarding APNs’ roles, their fields of application and their specific domain within the primary care system. Although the possibility to register as an APN — a protected title (https://www.apn-ch.ch) — is an important step, statutory parameters, for example regarding APNs’ reimbursement for their services, have yet to be established [10, 12]. Furthermore, little is known of how APN integration affects GPs’ classic roles. As a result, many GPs prefer to extend their collaborations with their medical assistants rather than forming new ones with APNs [13, 14].
However, as APNs’ scopes of practice differ substantially from those of medical assistants, their inclusion within GP practices affects GPs’ roles quite differently. For patients with chronic illness, the complexity of their conditions often requires not only clinical expertise but a holistic view of their needs [15, 16]. For example, APNs can successfully administer interventions aimed at behavioural change, which are well beyond the scope of medical practice coordinators or assistants [10, 17]. Accordingly, GPs can delegate numerous tasks to them. The occupational profiles of medical practice assistants and coordinators, and APNs are compared in table 1.
This study’s aim was to describe how APN integration affects GPs’ professional roles and GP-APN collaboration from the GPs' perspective. Its guiding question was, “How do GPs in a Swiss multiprofessional primary care practice experience the integration of APNs regarding changes in their own professional roles and their collaboration with APNs?"
Table 1Occupational profiles: medical practice assistant (MPA), medical practice coordinator (MPC), advanced practice nurse (APN).
| MPA | MPC | APN [9] |
| Professional training established in cooperation with GP | In Switzerland since 2015, module-based occupational advanced training | Master’s degree required, recognised in Switzerland since 2000 |
| Rule- and delegation-guided / Works in GP practice | Rule- and delegation-guided / Works in GP practice | Works autonomously as far as possible / Works internally and externally in relation to GP practices / Delegation (or substitution) of traditional medical duties with the goal of relieving GPs’ workload [11, 18, 19] / Supplementation of medical services / Complementary to GPs with the goal of holistic care (e.g., adherence fostering, consideration of psychosocial problems) [11, 18] |
| Support with administrative and technical duties (e.g., X-ray and laboratory) [13, 14] | Clinical emphasis: Consolidation of individual disease patterns / Goal: consultation, controls with stable or low-complexity patients (e.g., diabetes, wound care) | Elicits patient history / Assesses disease progression in chronically ill patients during house calls or rounds in care homes / Conducts clinical assessments / Induces first treatment steps in a close exchange with the GP or within a predetermined treatment schedule / Discerns emergency situations, consults GP in the case of complication or emergencies / Considers family and environment / Coordinates and considers involved services and institutions (e.g., home care, care homes) |
| Office executive emphasis: Team management / Personnel administration |
GP: general practitioner
The study site was a Swiss multiprofessional primary care practice. It has been working with APNs since 2011. In January 2020, the practice care team included 35 persons: 8 GPs, 19 medical practice assistants/coordinators and one APN, as well as 4 gynaecologists, 2 psychologists and 1 nutritionist. It had close ties to a number of medical specialists who provided examinations and consultations in the centre itself. All professions worked together as a multiprofessional team as part of one primary care centre.
This practice was the first in Switzerland to integrate an APN into its care team. The configuration of the APN role was initiated by the GPs, largely by delegating duties they had previously performed themselves to the APNs, especially regarding the care of chronically ill patients. At the time of this study, all necessary APN duties had been consolidated within the role of a nurse practitioner.
In addition to the tasks noted in our introduction, this nurse practitioner provided specific infusion therapy (immunotherapy) and complex wound care for patients visiting the practice. Although the practice employed only one nurse practitioner, other APNs working in three affiliated multiprofessional primary care practices had been trained here for several months before moving to their respective practices. Accordingly, GPs working in this practice had recent experience with various APNs.
This study was initiated by the first APN to be trained in this practice, who is now working in one of the care centre’s affiliated multiprofessional primary care practices and is a co-author of this study. She initiated this process when she approached the last author, a faculty member of the university where she did her Master’s degree, for advice on evaluating her APN practice outcomes. The current study is the first step of a broader project with the aim first of describing both physicians’ and APNs’ roles and competencies within the practice, then of deriving possible outcomes to evaluate. The current study focused on the physicians’ perspectives; the relevant APN roles and competencies were assessed in an ethnographic study and will be published separately.
This study employed a qualitative research design with a reflexive thematic analysis approach [20–23]. We oriented our efforts toward a social constructivist theory, which focuses on subjective experiences [24–25]. We chose this qualitative design because we were interested in the GPs’ experiences in working with APNs and their interpretation of those experiences. We wanted to understand the GPs' perspectives on the meaning of their professional roles and the changes therein, listening to how they constructed their GP-APN collaborations in their own words.
Using a purposive sampling approach, the APN who initiated the study recruited participants face-to-face and via email [26]. She approached each of the practice’s seven GPs and five affiliated specialists regarding possible participation. The inclusion criterion was at least 9 months of experience in collaboration with at least one APN working in the same multiprofessional primary care practice.
All invited medical specialists declined participation, as they had little interaction with the APNs. One GP declined participation for organisational reasons. Therefore, our sample included six GPs. The participants’ characteristics are presented in table 2.
Table 2Characteristics of individual participants.
| Participants | GPs (n = 6) | |
| Age | Average (SD) | 49 (12.2) |
| Range | 35–64 | |
| Gender | Male | 4 (66.7 %) |
| Female | 2 (33.3%) | |
| Highest educational achievement | University | 6 (100%) |
| Advanced training | Residency | 6 (100%) |
| Additional training | 1 (16.7%) | |
| Professional experience with APN | Average in years (SD) | 5.5 (2.8) |
| Range | 1.6-8.3 | |
| Professional experience total (current profession) | >20 years | 2 (33.3%) |
| 11–20 years | 3 (50%) | |
| 5–10 years | 1 (16.7%) | |
| 0–4 years | ||
APN: Advanced Practice Nurse; GP: general practitioner; SD: standard deviation
This study was conducted between August 2019 and February 2020. At that time, the first author was a Master’s student, building up her own APN role in a university hospital. She led individual semi-structured interviews with the practice’s participating GPs. Before the interviews, to help her understand the workings of the multiprofessional primary care practice, she also spent two days work-shadowing the recruiting APN. She scheduled one hour for each individual interview, which lasted from 28 to 53 minutes. A semi-structured interview guide with open-ended questions was used (see the appendix). Each interview started with the question of how the interviewed physician experienced everyday work in collaboration with the APN. Subsequent questions covered topics around changes in their everyday routines, tasks and roles, as well as their experiences from the beginning of their cooperation with APNs until the time of the interview.
All interviews were recorded as audio files and transcribed into standard German. The interview guide questions were adjusted based on the interviewer’s experiences in previous interviews. The interviewees demographic data were gathered via a questionnaire.
Data were analysed via reflexive thematic analysis, based on Braun and Clarke’s [21–23] six-phase method. During this iterative process, the complete dataset, including codes and themes, underwent several rounds of analysis, with movement back and forth between the various phases. For the coding process, we applied close-to-text coding of the physicians’ statements.
We used the GPs’ perspectives to generate potential themes and sub-themes. Each theme was generated around a core commonality, which we interpreted from our data. The detailed description of how we realised the six phases (following Braun and Clarke) are presented in table 3. Our analysis used MAXQDA (Version 2018, VERBI – Campus) to sort and organise the codes. To ensure methodological quality and consistency, a research team of two Master’s students and two senior researchers — all well-experienced in qualitative research — discussed the process in regular meetings. Interpretive discrepancies were discussed to produce the richest interpretations supported by the data. Additionally, interviews and analytical steps underwent ongoing critical reflection from a qualitative seminar group at the University of Basel.
Table 3Phases according to Braun and Clarke (2006).
| Realisation of the six phases according to Braun and Clarke (2006) | |
| Phase 1: Familiarisation with the data | After the transcription of the first two interviews, we started familiarising ourselves with the data by reading and re-reading them. |
| Phase 2: Coding | Once first patterns of meaning were identified through this process, we started coding. The Codes were discussed regularly within our research group. |
| New findings were integrated into the interview guide. | |
| Phase 3: Generating initial themes | We coded the entire dataset close to the transcribed texts and collated all codes to identify important features of our data. This process involved reading and re-reading the data multiple times. |
| The various codes were sorted to identify important patterns within the data. First, potential themes were generated. Codes and themes were continuously reviewed with the transcribed data and further developed with codes from the ongoing interviews. All themes were regularly discussed within our research and seminar groups. | |
| Phase 4: Reviewing themes | The initial themes were checked against the dataset. This involved reading and re-reading the data to determine whether the themes helped us to answer our research question and to interpret a compelling story from our data. |
| Phase 5: Defining and naming themes | To ensure coherence and consistency in terms of content, we conducted detailed analyses of all of our themes. Within the research group we named each theme. Each theme’s relationship to the research question was established. |
| Phase 6: Writing up | In the final phase, the first author wrote the scientific report and the final analysis. We chose data extracts that supported the themes. The report’s content and data extracts were regularly discussed within the research group. |
This study received clearance from the Ethics Commission of the Canton of Bern (Req-2019-00514). Informed consent was obtained before starting the interviews. All participation was voluntary, and all confidential information pseudonymised.
The analysis resulted in three main themes (fig. 1) concerning how GPs experienced the APN integration, particularly regarding changes in their own professional roles. Their experiences were as follows. (1) Trust as foundation for collaboration with APNs; trust is the most critical factor of how that collaboration affects their own roles. Trust allows the GPs (2) the build-up of the APN role by delegation, teaching, and supervision. GPs live their roles as delegators, shaping their own and the APN role by delegating tasks, as teachers by teaching towards delegation, and as supervisors, supporting the APNs in developing professional competencies, without which the new care model could not be built and maintained. Based on the trust built and the APN role developed, (3) GPs experience synergies of a partnership-based collaboration with APNs: APN involvement allows GPs a further development of their own GP role. Collaborating with APNs, GPs find added value for patients through high-quality care.
Figure 1 New Care Model: integration of an advanced practice nurse (APN) into general practitioner (GP) primary care.
In the first three years after starting working with APNs in 2011, the multiprofessional primary care centre’s GPs determined the general scope of APN practice. This provided a foundation upon which trust could be built. During this time, the practice’s GPs tailored APN duties to fit specific patient situations. Concurrently, intensive education modules were established and the APN’s competencies tested in diverse situations. As one GP commented, these measures were necessary to build mutual confidence between the physicians and the APNs:
"In the end, we bear the [medical] responsibility [...] and this is difficult in the beginning [...]: the trust has to be gained. But this will happen over time, as we get to know people." (GP)
Whereas the APN role could further develop and evolve over the following years, this initial establishment process did not need to be repeated. GPs who experienced this initial process emphasized that, for APNs joining the team later, it was clearly established which duties they would undertake and how they should proceed.
GPs named trust in the APN as essential for sound collaboration. Although the duration of trust building differed between GPs and remained a work in progress for some, all interviewed GPs expressed trust in the APN:
"I have and always have had complete trust in the APNs who worked with us." (GP)
They compared their experience of trust building with APNs with their experiences with other healthcare personnel. For example, whereas home-care workers tend to change jobs often — precluding the development of a trust base — the APN occupies a long-term position of trust for GPs. Additionally, most GPs already had experience working with and supervising junior doctors in hospital settings. As with those doctors, each APNs’ ability to clearly discern their personal abilities and limitations was an important basis for trust. One GP described this principle as follows:
"You can feel rather quickly whether trust is warranted, where the boundaries are or where more controls are in order [...]. They inspire more confidence — the APNs — than [...] many junior doctors."(GP)
Trust is the foundation of GPs’ collaboration with APNs. GPs’ confidence in individual APNs and their competencies determines which responsibilities they will delegate to them. This determines how GPs’ own professional roles are affected by the integration of APNs into their teams.
To promote the integration of APNs into their practice, GPs’ roles included safe delegation of duties to the APN, alongside teaching and supervision.
GPs remain legally liable and accountable for the care their patients receive, but they are confident that certain duties can be safely delegated to APNs. In the current organisation, as GPs individually decide what and how much to delegate, they also reshape their own roles.
Some specify only clearly distinguishable duties within structured treatment processes, such as infusion therapies for patients suffering from chronic autoimmune diseases, or duties in the care of more complex patients suffering from diabetes. To perform such tasks, APNs work independently within established treatment plans. Their “obligation to provide” includes checking with the responsible GP when patients’ test results fall outside normal ranges or when uncertainties/problems arise.
Some GPs preferred to delegate time-consuming duties that would otherwise interrupt the flow of their everyday practice, such as house calls. By referring to the APN’s feedback and laboratory results, they could diagnose problems and make treatment-related decisions. Another time-consuming routine duty delegated to APNs was administering Quick’s prothrombin time test.
Some GPs mentioned delegating tasks in the context of nursing home residents. There, APNs could relieve GPs, for example by collecting necessary resident data — leaving GPs time to focus on adjusting medications in acute situations without examining all residents personally. In addition to scheduling check-up visits as necessary, APNs organised communication and coordinated care activities both with the facility and with residents’ families.
"The APN examines residents of a care home [...] where she provides regular control visits and reports to me afterwards, if there are problems." (GP)
GPs who preferred more direct contact with their nursing home patients — relationships with whom they had commonly developed over a span of many years — shaped their delegation differently. One GP considered some patients almost like family members. In such cases, having personally monitored those patients’ conditions for decades, he found it difficult to delegate that task.
GPs also delegated patient case management to APNs, who also provided much direct care, for example during house calls or rounds in care homes. Where case management was delegated, it was supervised with varying degrees of stringency. Some GPs checked on their patients’ progress via the data the APNs entered into their files after each care visit. Others informed themselves before each visit about scheduled examinations.
"I get every record of the regular [care home] control visits [...] [from the APN]; therefore, I am always up-to-date and of course I get every laboratory result.” (GP)
Although the selection of delegated tasks was physician-dependent, the care centre reviewed the division of responsibilities via semi-annual APN-GP patient conferences. During these, concrete patient situations were analysed to optimise the division of responsibilities.
To ensure that APNs acquired the competencies necessary to execute all delegated duties, appropriate teaching and training were necessary. With the integration of an APN, the GPs’ roles included teaching and supervision. Particularly in the early stages of collaboration, instruction was provided systemically. One GP noted that, when new APNs first arrived, they were trained intensively to gather clinical data to the level necessary to assume those GP duties.
"When we provided medical services for a large care home, we also provided medical consultation hours there. [...] [The APN] had to ascertain patient histories herself, as well as do examinations and report to me afterwards, like a junior doctor in a hospital." (GP)
These GPs, who were already accustomed to collaborating with junior physicians, shifted their teaching roles to the APNs. One GP, a former chief resident, recalled that they were happy to be teaching again. Others declared that this extra training allowed them to delegate more duties to the APNs. Over the years, the amount of teaching had declined somewhat; however, it remained a vital element of collaboration.
The central purpose of supervision within the GP-APN collaboration was to support the APNs in developing professional competencies and optimising operational procedures. The APNs would meet the GPs in charge when support was necessary or to ascertain how to proceed with various patient situations. This was especially important when collaborating with new GPs:
"[By] actually assessing patients together, [...] I relatively quickly develop [...] an impression as to how advanced they are in clinical assessment." (GP)
The effort of teaching and supervision within the first months of collaboration was large, but declined substantially over time. The possibility of delegating tasks to the APNs offered the GPs relief from routine, time-intensive duties, freeing them for other activities.
All GPs described experiencing partnership-based synergies when working with APNs. By enriching their own roles, they perceived that they were able to offer more comprehensive, high-quality patient care.
Most of the interviewed GPs used the time the APNs saved them to concentrate more on core tasks, to further develop their own competencies or to add depth to their existing patient relationships. One mentioned that they gladly continued to provide house calls to certain patients not regularly cared for at home. Another appreciated that their increased availability during consultation hours allowed them to respond to problems that might not otherwise have received the needed attention. Still others used the time gained to obtain further education in diagnostics and surgery, i.e., to increase their competencies. One GP remarked that this made their work as a GP more exciting:
"This adds value to everyday life [...] These are all things you can do manually [...]. Be it punctures, be it ultrasound or surgery [...], it is tremendously satisfying if you achieve results rather swiftly by manual labour." (GP)
A small number of GPs experienced little synergy — for instance, if communication with an APN required large amounts of time:
"To always just answer questions in the background, at the computer [...] can be a little frustrating; because essentially I like to be in contact with patients." (GP)
All participating GPs saw added value for their patients in their interprofessional collaboration with APNs. GPs mentioned that, by improving networks and coordination of players within the healthcare system, this collaboration benefited patients from various perspectives. On the one hand, more time was available for patient care; on the other, the GPs’ knowledge and experience coalesced well with those of the APNs.
Some GPs also recognised that their collaboration with APNs enabled them to provide additional services to their patients. For example, patients no longer need to be sent to distant central hospitals for time-consuming tests, which is highly valued by chronically ill patients. One example of a treatment that demanded high-level competencies and was offered within the multiprofessional primary care practice was intravenous immunoglobulin (IVIG) therapy:
"[IVIG] demands adequate experience [...]. These are issues where, in a regular case, a semi-stationary or stationary day clinic would be employed." (GP)
Several GPs described how they could assure chronically ill patients high-quality house calls and care home rounds through the aid of APNs. APNs and GPs worked in close contact, sharing responsibility for patients’ care. And when a patient’s health situation changed, most GPs would discuss further treatment steps with the APN:
"With one older patient, who in the end really lived on her own for a very, very long time, suffering from grave cardiomyopathy, which proved a delicate adjustment [...]. There, [an APN] did the regular house calls." (GP)
Some GPs emphasised the APNs’ holistic perspective. The patients appreciated this very much — for instance, the support APNs provided in handling the effects of illness. Because APNs are trained to care regularly for patients over a long period, they build familiarity with all participating healthcare services and institutions, with an eye to coordinating their duties.
For this study, we describe the experiences of GPs in a Swiss multiprofessional primary care practice concerning the integration of APNs into their patient care team with respect to their own professional roles. Our findings show that trust in the APN was the basis for delegation and guided the content of the GPs’ role changes. In the beginning, a time investment was necessary for the GPs to teach and supervise the APNs. With time, though, GPs experienced synergies when working with APNs, as the delegation of tasks freed up time for other activities of their choosing. One particular added value was the increase in comprehensive, high-quality patient care.
Physicians bear responsibility for all medical procedures entrusted to them — including those not executed personally [27]. Therefore, one essential prerequisite for the delegation of duties was the GPs’ full trust in the APN. Overall, this trust took time to build and developed on an individual basis.
Further, not only the APNs’ competencies per se, but the clear acknowledgement of the limits of those competencies, were considered critical for functional collaborations. This is congruent with the findings of several previous studies that acknowledgement of professional competencies is a critical step towards constructing a trust base. For example, Blue and Fitzgerald [28] showed that trust could develop only after GPs understood the APNs’ competencies. Even where trust-building is underway, various studies have illustrated that, alongside acknowledgement of job competencies, high-quality collaboration demands mutual respect. If strong professional competencies do not cultivate respect, they may instead sow frustration and mistrust, hindering the development of trust [29, 30]. Without trust, GPs cannot delegate duties to APNs; instead, they must deal with the surplus of controls of APNs’ tasks [30–32]. Such cases benefit neither the GP nor the APN: the GP continues to spend time on matters such as basic clinical assessments that others delegate fully to APNs; and the APN does not develop professionally by learning and performing those tasks.
One step towards fostering acceptance and acknowledgement of APNs’ professional competencies among GPs is to align those competencies with international standards during the APN training process. In recent years, Swiss universities and universities of applied sciences with clinical mentoring programmes, for example, the Universities of Basel and Lausanne [33], have begun expanding their APN programmes’ clinical practice content. Their APN clinical mentorship programmes include training in various clinical assessment and examination techniques. Providing newly certified APNs with readily applicable professional competencies during their education readies them to relieve common GP duties with minimal GP input after they join practices. Naturally, practice-specific competencies still require focused training and supervision.
This study’s GPs recalled that during their early collaboration with APNs, they invested considerable time and effort with little immediate relief. However, intensive teaching and supervision in the early stages ensured safe patient care. Over time, they reduced the amount of teaching and supervision. This reflects not only new APNs’ growing repertoire of clinically competencies, but also the fact that, in recent years, part of their initial training has been taken over by more experienced APNs.
Previous researchers have observed that the introduction of a newly-hired APN can take from three months to three years. This initial learning period depends partly on the APN’s previous education and professional experience and partly on the GP’s experience with this kind of collaboration [30, 32–34]. GPs consider teaching and supervision of APNs central to the quality and safety of patient care [30, 35–37].
Every studied GP decided individually which duties to delegate. These decisions also shaped their own professional roles. Whereas duties are generally delegated within structured treatment processes, very time-consuming ones may be handled individually. Patient care, house calls or the treatment of care home residents involves delegating entire sets of responsibilities, which can include case management. Several studies have also described how GPs can lighten their case management duties via delegation, for example, where treatment standards and predefined processes exist or patient groups are well-defined [38, 39].
In the Swiss Health Observatory’s report on the inclusion of highly educated non-medical professional personnel to Swiss primary medical care practices [10], a group of Swiss experts supported the allocation of chronically ill patients’ case management to APNs. According to them, numerous tasks relating to this patient group’s care do not specifically require a GP’s knowledge and skills.
Several studies have established that GPs experience numerous synergies as a result of interprofessional collaboration with APNs, particularly where they delegate tasks that the APNs can effectively and efficiently fulfil [10, 36, 40]. This type of collaboration implies that the GP will no longer meet regularly with all patients treated within the scope of their practice. Similarly, it is assumed that the GP will take on the roles of interprofessional care team leader, supervisor and clinical mentor to the APN. Accordingly, several studies have confirmed that, especially regarding treatment of patients with complex health needs, interprofessional collaboration with APNs relieves GPs’ workloads considerably [32, 35, 39].
This workload reduction was appreciated most as shown in another Swiss study [41]. Norful, de Jacq, Carlino and Poghosyan indicated that, as reducing GPs’ workload also reduced the emotional burden of their work, it would likely also reduce their incidence of burnout [42]. Our results confirmed that, when APNs carried out house calls and care home rounds, the interviewed GPs perceived such input as a tremendous relief. Such care tasks are extremely time-consuming and entail major interruptions in GPs’ daily practice.
Furthermore, our analyses indicated that the degree of workload relief depended partly on the balance between supervised and autonomous duties delegated to the APN. This observation supports the results of several leading studies. The reason is straightforward: regardless of the APN’s mounting experience, if the time and effort devoted to supervision and communication did not decrease over time, the GP achieved no net relief [30–32, 38].
In partnership-based collaborations with APNs, our data confirmed that the GPs who enlisted APNs received considerable net added value. They could use their freed-up time to concentrate on highly complex medical cases and learn or develop other competencies. In this respect, most GPs experienced additional work value through development of their own competencies. These results echo those of previous studies: Collaborating with APNs allowed GPs opportunities to develop professionally, to offer new services or simply to care for more patients [32, 43]. Several GPs particularly appreciated APNs’ input regarding their management of patients’ psychosocial needs [32].
GPs emphasised their joint capacity to ensure high-quality care through collaboration with APNs on house calls and caring for chronically ill patients in care homes. In fact, a large share of the practice’s contact with homecare and care home residents was performed by APNs. For the GPs, the APNs’ emphasis on continuity of care meant complications could be discerned and timely preventive measures provided, thereby minimising hospitalizations. In such cases, GP-APN collaborations provided the quality of care necessary for patients to remain living at home. This observation supports those of various studies confirming APNs’ ability to provide high-quality, efficient care to chronically ill patients [10, 40, 44].
As indicated in our GP interviews, the study practice’s APNs also focused on duties for which GPs had little time. These included coordination of and communication with the many health services involved in patient care. As APNs can devote more time to individual patients’ care than GPs, they can also focus on issues such as mastering activities of daily living, infection prevention and therapy adherence. This supports the findings of several previous studies, for example, describing GPs’ sense of relief when APNs were able to focus on functions the GPs never felt they could fulfill satisfactorily themselves, such as the delivery of behavioural or psychosocial interventions [30, 33, 44]. One Dutch study [43] emphasised APNs’ opportunity to invest far more time than GPs in patient care, allowing them to bring a more holistic perspective into the care process.
This qualitative research study had certain notable limitations. On the one hand, our sample was limited to six GPs from a single multiprofessional practice. Therefore, our findings cannot be generalised to Swiss primary care practices overall. However, other GPs might relate to the experiences described here and profit from the lessons learned in integrating APNs into primary and geriatric care practices. Also, the translation of the quotations into English might have affected the original meaning; and the researchers and their background may impact their interpretation of the data: Most of the authors of this paper are nurses, four are APNs, one is a GP. All are convinced that the studied model of GP-APN collaboration adds value and that the practice provides a positive example of APN integration.
Interprofessional GP models with APNs are tremendously promising, offering new possibilities for efficient, high-quality patient care. In close collaboration with GPs, APNs are especially well-suited to work with multimorbid patients with complex care needs in their own homes or care homes. These capacities are well-supported by evidence of their effectiveness and efficiency. The care model examined in the current study is particularly promising, as it can easily be adapted for implementation in other settings.
Supporting the dissemination of care models integrating APNs within Swiss primary health care will require the improvement of certain general conditions. Among others, these include the discernment of a distinct legal status for Advanced Practice Nursing as a profession and provisions for the financial compensation of APNs by health insurers, as well as reimbursement of GPs for the mentoring they provide. One important step recently taken in Switzerland was the registration of the professional APN role by the Association APN-CH.
The authors like to thank all participants for their valuable contribution to this study.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest was disclosed.
We have no financial support for this work to declare.
1. Schweizerische Gesundheitsdirektorenkonferenz und Bundesamt für Gesundheit . Neue Versorgungsmodelle für die medizinische Grundversorgung. Bericht der Arbeitsgruppe „Neue Versorgungsmodelle für die medizinische Grundversorgung“ von GDK und BAG. Bern; 2012.
2. Senn N , Ebert ST , Cohidon C . Die Hausarztmedizin in der Schweiz –Perspektiven. Analyse basierend auf den Indikatoren des Programms SPAM (Swiss Primary Care Active Monitoring). Obsan Bulletin 11/2016. Neuchâtel (Switzerland): Schweizerisches Gesundheitsobservatorium. 2016.
3. Hostettler S , Kraft E . FMH-Ärztestatistik 2017 –aktuelle Zahlen. Schweiz Arzteztg. 2018;99(13–14):408–13.
4. Seematter-Bagnoud L , Junod J , Jaccard Ruedin H , Roth M , Foletti C , Santos-Eggimann B . Offre et recours aux soins médicaux ambulatoires en Suisse – Projections à l’horizon 2030. [Supply and use of ambulatory care in Switzerland – Projections for 2030]. Neuchâtel (Suisse): Observatoire Suisse de la Santé; 2008. (Document de travail 33).
5. Kilpatrick K , Kaasalainen S , Donald F , Reid K , Carter N , Bryant-Lukosius D , et al. The effectiveness and cost-effectiveness of clinical nurse specialists in outpatient roles: a systematic review. J Eval Clin Pract. 2014 Dec;20(6):1106–23. https://doi.org/10.1111/jep.12219
6. Laurant M , Reeves D , Hermens R , Braspenning J , Grol R , Sibbald B . Substitution of doctors by nurses in primary care. Cochrane Database Syst Rev. 2005 Apr;(2):CD001271. https://doi.org/10.1002/14651858.CD001271.pub2
7. Martin-Misener R , Harbman P , Donald F , Reid K , Kilpatrick K , Carter N , et al. Cost-effectiveness of nurse practitioners in primary and specialised ambulatory care: systematic review. BMJ Open. 2015 Jun;5(6):e007167. https://doi.org/10.1136/bmjopen-2014-007167
8. Martínez-González NA , Djalali S , Tandjung R , Huber-Geismann F , Markun S , Wensing M , et al. Substitution of physicians by nurses in primary care: a systematic review and meta-analysis. BMC Health Serv Res. 2014 May;14(1):214. https://doi.org/10.1186/1472-6963-14-214
9. International Council of Nurses . Guidelines on advanced practice nursing. 20120
10. Künzi K , Jäggi J , Dutoit L . Aktueller Stand der schweizerischen Diskussion über den Einbezug von hoch ausgebildeten nichtärztlichen Berufsleuten in der medizinischen Grundversorgung [Current status of the Swiss debate on the involvement of highly trained non-medical professional people in primary care: Update on the Working Document 27 Schlussbericht Obsan]. Neuchâtel (Switzerland): Schweizerisches Gesundheitsobservatorium. 2013.
11. Maier C , Aiken L , Busse R . Nurses in advanced roles in primary care: Policy Levers for Implementation. Health Working Papers. Paris: OECD Publishing. 2017.
12. Kieser U . Advanced Practice Nurse and Clinical Nurse Specialist - neue Entwicklungen bei Pflegefachpersonen. Pflegerecht. 2016;5(3):130–41.
13. Huber F . Empowerment für MPAs: bedeutung für den Hausarzt. PrimaryCare. 2012;12(23):447. https://doi.org/10.4414/pc-d.2012.00192
14. Schalch E . Nurse Practitioner oder Medizinische Praxiskoordinatorin? Schweiz Arzteztg. 2011;92(43):1665–7. https://doi.org/10.4414/saez.2011.16395
15. De Geest S , Moons P , Callens B , Gut C , Lindpaintner L , Spirig R . Introducing Advanced Practice Nurses / Nurse Practitioners in health care systems: a framework for reflection and analysis. Swiss Med Wkly. 2008 Nov;138(43-44):621–8.
16. Gaidys U . Qualität braucht Kompetenz und Verantwortung - Herausforderungen und Perspektiven einer Advanced Nursing Practice für die Gesundheitsversorgung aus pflegewissenschaftlicher Sicht. Pflege. 2011 Feb;24(1):15–20. https://doi.org/10.1024/1012-5302/a000087
17. Gysin S , Odermatt M , Merlo C , Essig S . Pflegeexpertinnen APN und ¬Medizinische Praxiskoordinatorinnen in der Hausarztpraxis. Prim Hosp Care. 2020;20(01):19–22. https://doi.org/10.4414/phc-d.2020.10137
18. Djalali S , Rosemann T . Neue Versorgungsmodelle für chronisch Kranke. Hintergründe und Schlüsselelemente (Obsan Dossier 45). Neuchâtel (Switzerland): Schweizerisches Gesundheitsobservatorium. 2015.
19. World Health Organization . Task shifting: Rational Redistribution of Tasks among Health Workforce Teams: Global Recommendations and Guidelines. 2007, Geneva, Switzerland: WHO
20. Creswell JW . Research design. Qualitative and Quantitative Approach 5th ed. Thousand Oaks: SagePublications; 2018.
21. Braun V , Clarke V . Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. https://doi.org/10.1191/1478088706qp063oa
22. Braun V , Clarke V . Successful qualitative research: A practical guide for beginners. London: Sage; 2013.
23. Braun V , Clarke V . Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–97. https://doi.org/10.1080/2159676X.2019.1628806
24. Berger P , Luckmann T . The social construction of reality. London: Penguin Books; 1991.
25. Burr V . Social constructionism 2nd ed. London: Routledge; 2003.
26. Tongco MD . Purposive sampling as a tool for informant selection. Ethnobot Res Appl. 2007;5:147–58. https://doi.org/10.17348/era.5.0.147-158
27. Schweizerische Akademie der Medizinischen Wissenschaften, Swiss Medical Association, editor . Rechtliche Grundlagen im medizinischen Alltag. Ein Leitfaden für die Praxis. 2. Auflage. Muttenz: Schwabe; 2013.
28. Blue I , Fitzgerald M . Interprofessional relations: case studies of working relationships between Registered Nurses and general practitioners in rural Australia. J Clin Nurs. 2002 May;11(3):314–21. https://doi.org/10.1046/j.1365-2702.2002.00591.x
29. Pullon S . Competence, respect and trust: key features of successful interprofessional nurse-doctor relationships. J Interprof Care. 2008 Mar;22(2):133–47. https://doi.org/10.1080/13561820701795069
30. Andregård AC , Jangland E . The tortuous journey of introducing the nurse practitioner as a new member of the healthcare team: a meta-synthesis. Scand J Caring Sci. 2015 Mar;29(1):3–14. https://doi.org/10.1111/scs.12120
31. Aerts N , Van Bogaert P , Bastiaens H , Peremans L . Integration of nurses in general practice: A thematic synthesis of the perspectives of general practitioners, practice nurses and patients living with chronic illness. J Clin Nurs. 2020 Jan;29(1-2):251–64. https://doi.org/10.1111/jocn.15092
32. Schadewaldt V , McInnes E , Hiller JE , Gardner A . Views and experiences of nurse practitioners and medical practitioners with collaborative practice in primary health care - an integrative review. BMC Fam Pract. 2013 Sep;14(1):132. https://doi.org/10.1186/1471-2296-14-132
33. Bischofberger I , Käppeli A , Essig S , Gysin S . Klinisches Mentorat für Pflegeexpertinnen und -experten MSC. Schweiz Arzteztg. 2020;101(07):204–6. https://doi.org/10.4414/saez.2020.18599
34. Contandriopoulos D , Brousselle A , Dubois CA , Perroux M , Beaulieu MD , Brault I , et al. A process-based framework to guide nurse practitioners integration into primary healthcare teams: results from a logic analysis. BMC Health Serv Res. 2015 Feb;15(1):78. https://doi.org/10.1186/s12913-015-0731-5
35. Lindblad E , Hallman EB , Gillsjö C , Lindblad U , Fagerström L . Experiences of the new role of advanced practice nurses in Swedish primary health care—a qualitative study. Int J Nurs Pract. 2010 Feb;16(1):69–74. https://doi.org/10.1111/j.1440-172X.2009.01810.x
36. Read S . Nursing UoSSo, Midwifery. Exploring New Roles in Practice (ENRiP): Final Report. University of Sheffield, School of Nursing and Midwifery; 2001.
37. American Medical Directors Association Ad Hoc Work Group on the Role of the Attending Physician and Advanced Practice Nurse . Collaborative and supervisory relationships between attending physicians and advanced practice nurses in long-term care facilities. Geriatr Nurs. 2011 Jan-Feb;32(1):7–17. https://doi.org/10.1016/j.gerinurse.2010.12.010
38. Niezen MG , Mathijssen JJ . Reframing professional boundaries in healthcare: a systematic review of facilitators and barriers to task reallocation from the domain of medicine to the nursing domain. Health policy (Amsterdam, Netherlands). 2014;117(2):151-69.
39. Jakimowicz M , Williams D , Stankiewicz G . A systematic review of experiences of advanced practice nursing in general practice. BMC Nurs. 2017 Jan;16(1):6. https://doi.org/10.1186/s12912-016-0198-7
40. Laurant M , van der Biezen M , Wijers N , Watananirun K , Kontopantelis E , van Vught A . Nurses as substitutes for doctors in primary care. Cochrane Database of Systematic Reviews. 2018(7).
41. Gysin S , Sottas B , Odermatt M , Essig S . Advanced practice nurses’ and general practitioners’ first experiences with introducing the advanced practice nurse role to Swiss primary care: a qualitative study. BMC Fam Pract. 2019 Nov;20(1):163. https://doi.org/10.1186/s12875-019-1055-z
42. Norful AA , de Jacq K , Carlino R , Poghosyan L . Nurse Practitioner-Physician Comanagement: A Theoretical Model to Alleviate Primary Care Strain. Ann Fam Med. 2018 May;16(3):250–6. https://doi.org/10.1370/afm.2230
43. van der Biezen M , Derckx E , Wensing M , Laurant M . Factors influencing decision of general practitioners and managers to train and employ a nurse practitioner or physician assistant in primary care: a qualitative study. BMC Fam Pract. 2017 Feb;18(1):16. https://doi.org/10.1186/s12875-017-0587-3
44. Dick K , Frazier SC . An exploration of nurse practitioner care to homebound frail elders. J Am Acad Nurse Pract. 2006 Jul;18(7):325–34. https://doi.org/10.1111/j.1745-7599.2006.00140.x
The appendix is available in the pdf version of this article.