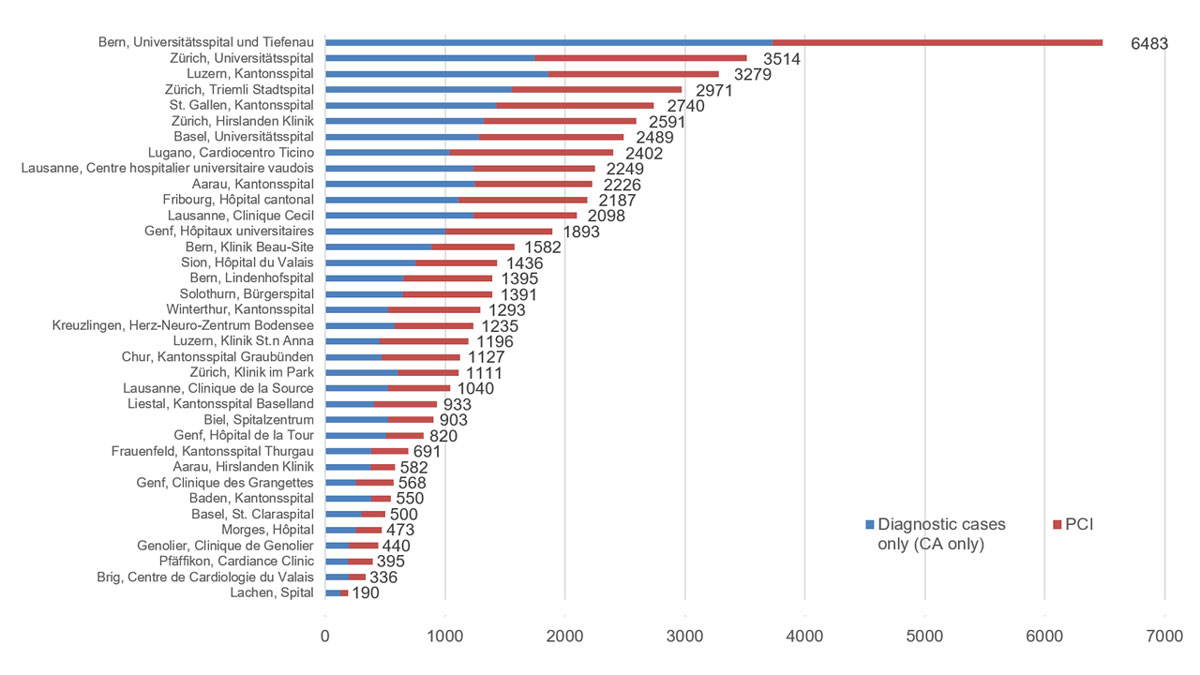
Figure 1 Percutaneous coronary interventions (PCI) during the year 2018 in Switzerland. CA = coronary angiography
DOI: https://doi.org/10.4414/smw.2020.20200
Cardiovascular diseases including coronary artery disease and structural heart disease are still the main causes of hospitalisations and medical consultations worldwide. Despite improvements in the management of patients with cardiovascular diseases, they remain life-threatening disorders [1–3]. In Switzerland, the entire population (permanent residents, periodic residents, as well as tourists) have an unrestricted access to emergency care and high-quality, evidence-based medicine, and health costs are covered by compulsory insurance. Individuals who cannot afford to pay health insurance fees are subsidised by the government.
In this scenario, the Working Group Interventional Cardiology of the Swiss Society of Cardiology performs a nationwide annual survey on percutaneous cardiac procedures in adults based on aggregate data provided by each institution. Since 1987, and based on a standardised questionnaire that has evolved over the years, all cardiology centres are asked to report yearly aggregate data on the number and type of procedures performed [4]. Since 2008, data have been published on the website of the Swiss Working Group for Interventional Cardiology of the Swiss Society of Cardiology and several publications emerged from these data [5–8].
All interventional centres in Switzerland were asked to participate and to fill in an online questionnaire or electronic data sheets containing important items that mirror current interventional activities. In our current version of the questionnaire, 71 items are covered: information on infrastructure, numbers of operators, availability of on-site cardiac surgery, numbers of coronary angiography investigations (CAs) and percutaneous coronary interventions (PCIs) (stratified for ST-segment elevation myocardial infarction [STEMI], non-ST-segment elevation acute coronary syndromes [NSTE-ACS], cardiogenic shock or cardiac arrest and stable coronary disease [CAD]), access site, specific revascularisation techniques (e.g., rotational atherectomy, recanalisation of chronic totally occluded vessels [CTO]), adjunctive techniques (e.g., use of intravascular imaging, distal protection devices) and use of mechanical circulatory support. Among structural heart interventions, information was available on balloon valvuloplasties, transcatheter aortic valve implantation (TAVI), percutaneous mitral-, tricuspidal- or pulmonary-valve interventions, closure of shunts, as well as of paravalvular leaks and left atrial appendage (LAA) occlusion, transcoronary ablation of septal hypertrophy (TASH), pericardial drainage, catheter-based therapies of pulmonary embolism, coronary sinus reduction, and interventional renal denervation. Finally, data on in-hospital mortality for PCIs were gathered and stratified according to the clinical presentation (STEMI, NSTE-ACS, stable CAD and cardiac arrest/cardiogenic shock).
Data were aggregated and displayed using standard software. There was no formal statistical analysis. Since data collection and analysis were for quality assurance/control purposes only for in-hospital mortality after interventional procedures, no formal approval by local institutional review boards and/or written patient consent is required.
In 2018, there were 36 interventional centres located in 17 of the 26 Swiss cantons: 5 university hospitals, 15 non-university public hospitals and 16 private institutions. All 36 centres provided local data on their performances in 2018.
All centres performed both diagnostic and therapeutic procedures and 16 (43%) had on-site cardiac surgery (table 1). During 2018, 57,309 CAs and 27,318 PCIs were performed by 224 PCI operators and 37 operators performing diagnostic CA only (fig. 1). The median PCI/CA ratio was 47% with a range from 32 to 62% (table 2). Figure 1 displays the distribution of CA and PCIs among the different centres in 2018. The average number of CAs per operator was 220 cases/year and the average number of PCIs per operator was 122 cases/year (tables 1 and 2 ). With regard to access sites, the femoral and the radial artery were used almost equally often in all institutions together (53 vs 47%, respectively) with a wide range from 16 to 98% among the centres (table 3, fig. 2).
Table 1 Characteristics of the centres included.
| Centre | Clinic description | Canton | Number of catheter labs | PCI operators | Operators diagnostic only | Cardiac surgery onsite |
|---|---|---|---|---|---|---|
| Aarau, Hirslanden Klinik | Non-university community centre | Aargau | 2 | 14 | – | Yes |
| Aarau, Kantonsspital | Non-university community centre | Aargau | 2 | 5 | 5 | No |
| Baden, Kantonsspital | Non-university community centre | Aargau | 1 | 5 | – | No |
| Basel, St. Claraspital | Private clinic | Basel-Stadt | 1 | 3 | – | No |
| Basel, Universitätsspital | University centre | Basel-Stadt | 2 | 8 | 1 | Yes |
| Bern, Klinik Beau-Site | Private clinic | Bern | 2 | 7 | – | Yes |
| Bern, Lindenhofspital | Private clinic | Bern | 2 | 4 | 3 | No |
| Bern, Universitätsspital und Tiefenau | University centre | Bern | 4 | 11 | – | Yes |
| Biel, Spitalzentrum | Non-university community centre | Bern | 1 | 5 | – | No |
| Brig, Centre de Cardiologie du Valais | Private clinic | Wallis | 1 | 3 | – | No |
| Chur, Kantonsspital Graubünden | Non-university community centre | Graubünden | 1 | 4 | – | No |
| Frauenfeld, Kantonsspital Thurgau | Non-university community centre | Thurgau | 1 | 6 | 1 | No |
| Fribourg, Hôpital cantonal | Non-university community centre | Freiburg | 1 | 5 | – | No |
| Genf, Clinique des Grangettes | Private clinic | Genf | 1 | 4 | 3 | No |
| Genf, Hôpital de la Tour | Private clinic | Genf | 2 | 8 | 3 | Yes |
| Genf, Hôpitaux universitaires | University centre | Genf | 2 | 5 | – | Yes |
| Genolier, Clinique de Genolier | Private clinic | Waadt | 1 | 4 | – | No |
| Kreuzlingen, Herz-Neuro-Zentrum Bodensee | Private clinic | Thurgau | 1 | 7 | – | Yes |
| Lachen, Spital | Non-university community centre | Schwyz | 1 | 6 | 1 | No |
| Lausanne, Centre hospitalier universitaire vaudois | University centre | Waadt | 2 | 6 | – | Yes |
| Lausanne, Clinique Cecil | Private clinic | Waadt | 1 | 17 | 11 | Yes |
| Lausanne, Clinique de la Source | Private clinic | Waadt | 1 | 4 | 1 | No |
| Liestal, Kantonsspital Baselland | Non-university community centre | Basel-Landschaft | 1 | 2 | – | No |
| Lugano, Cardiocentro Ticino | Non-university community centre | Tessin | 4 | 9 | 1 | Yes |
| Luzern, Kantonsspital | Non-university community centre | Luzern | 2 | 5 | – | Yes |
| Luzern, Klinik St. Anna | Private clinic | Luzern | 1 | 5 | 1 | No |
| Morges, Hôpital | Non-university community centre | Waadt | 1 | 4 | 4 | No |
| Pfäffikon, Cardiance Clinic | Private clinic | Schwyz | 1 | 3 | 1 | No |
| Sion, Hôpital du Valais | Non-university community centre | Wallis | 2 | 5 | – | Yes |
| Solothurn, Bürgerspital | Non-university community centre | Solothurn | 1 | 4 | – | No |
| St. Gallen, Kantonsspital | Non-university community centre | St. Gallen | 3 | 8 | – | No |
| Winterthur, Kantonsspital | Non-university community centre | Zürich | 2 | 5 | – | No |
| Zürich, Hirslanden Klinik | Private clinic | Zürich | 2 | 12 | – | Yes |
| Zürich, Klinik im Park | Private clinic | Zürich | 2 | 6 | 1 | Yes |
| Zürich, Triemli Stadtspital | Non-university community centre | Zürich | 2 | 7 | – | Yes |
| Zürich, Universitätsspital | University centre | Zürich | 2 | 8 | – | Yes |
| Total | 17 | 59 | 224 | 37 | 16 | |
PCI = percutaneous coronary intervention
Figure 1 Percutaneous coronary interventions (PCI) during the year 2018 in Switzerland. CA = coronary angiography
Table 2 Characteristics of the coronary interventions: number of cases and indications.
| Centre |
Total number of cases
(CA + PCI) |
Diagnostic cases only
(CA only) |
PCI | % PCI per CA | PCI for NST-ACS | PCI for STEMI | PCI for cardiogenic shock / cardiac arrest | PCI for CTO | Antegrade CTO | Retrograde CTO |
|---|---|---|---|---|---|---|---|---|---|---|
| Aarau, Hirslanden Klinik | 582 | 377 | 205 | 35% | 32 | 17 | 3 | 15 | 15 | – |
| Aarau, Kantonsspital | 2226 | 1249 | 977 | 44% | 311 | 238 | 23 | 129 | 117 | 12 |
| Baden, Kantonsspital | 550 | 384 | 166 | 30% | 82 | – | – | 21 | 21 | – |
| Basel, St. Claraspital | 500 | 301 | 199 | 40% | 25 | 8 | 1 | 6 | 6 | – |
| Basel, Universitätsspital | 2489 | 1281 | 1208 | 49% | 296 | 272 | 90 | 64 | 56 | 8 |
| Bern, Klinik Beau-Site | 1582 | 884 | 698 | 44% | 92 | 46 | – | n.a. | n.a. | n.a. |
| Bern, Lindenhofspital | 1395 | 655 | 740 | 53% | 92 | 64 | 87 | 10 | 10 | – |
| Bern, Universitätsspital und Tiefenau | 6483 | 3732 | 2751 | 42% | 815 | 526 | 88 | 157 | – | – |
| Biel, Spitalzentrum | 903 | 524 | 379 | 42% | 153 | 90 | 6 | 19 | 15 | 4 |
| Brig, Centre de Cardiologie du Valais | 336 | 196 | 140 | 42% | 1 | – | – | 20 | 20 | – |
| Chur, Kantonsspital Graubünden | 1127 | 474 | 653 | 58% | 178 | 154 | 5 | 51 | 44 | 7 |
| Frauenfeld, Kantonsspital Thurgau | 691 | 386 | 305 | 44% | 63 | 4 | – | 11 | 11 | 1 |
| Fribourg, Hôpital cantonal | 2187 | 1111 | 1076 | 49% | 198 | 141 | 17 | 178 | 178 | 2 |
| Genf, Clinique des Grangettes | 568 | 255 | 313 | 55% | 13 | 2 | – | 23 | 18 | 5 |
| Genf, Hôpital de la Tour | 820 | 508 | 312 | 38% | 41 | 20 | – | 16 | 12 | 4 |
| Genf, Hôpitaux universitaires | 1893 | 1001 | 892 | 47% | 123 | 229 | 20 | 52 | n.a. | n.a. |
| Genolier, Clinique de Genolier | 440 | 199 | 241 | 55% | – | 2 | – | 5 | 4 | 1 |
| Kreuzlingen, Herz-Neuro-Zentrum Bodensee | 1235 | 578 | 657 | 53% | 87 | 42 | 18 | 21 | 21 | – |
| Lachen, Spital | 190 | 130 | 60 | 32% | 7 | – | – | 4 | 4 | – |
| Lausanne, Centre hospitalier universitaire vaudois | 2249 | 1233 | 1016 | 45% | 381 | 298 | 18 | 54 | 40 | 14 |
| Lausanne, Clinique Cecil | 2098 | 1234 | 864 | 41% | 38 | 1 | – | 47 | n.a. | n.a. |
| Lausanne, Clinique de la Source | 1040 | 522 | 518 | 50% | 49 | – | – | 52 | 52 | – |
| Liestal, Kantonsspital Baselland | 933 | 406 | 527 | 56% | 174 | 54 | 8 | 81 | 56 | 25 |
| Lugano, Cardiocentro Ticino | 2402 | 1037 | 1365 | 57% | 293 | 227 | 30 | 31 | 28 | 3 |
| Luzern, Kantonsspital | 3279 | 1858 | 1421 | 43% | 273 | 388 | 99 | 177 | 135 | 42 |
| Luzern, Klinik St. Anna | 1196 | 453 | 743 | 62% | 62 | 38 | 19 | 40 | 32 | 8 |
| Morges, Hôpital | 473 | 255 | 218 | 46% | 67 | 1 | – | 14 | 12 | 2 |
| Pfäffikon, Cardiance Clinic | 395 | 193 | 202 | 51% | 34 | 1 | – | 12 | 12 | – |
| Sion, Hôpital du Valais | 1436 | 749 | 687 | 48% | 225 | 165 | 15 | 25 | 20 | 5 |
| Solothurn, Bürgerspital | 1391 | 648 | 743 | 53% | 305 | 134 | – | – | – | – |
| St. Gallen, Kantonsspital | 2740 | 1426 | 1314 | 48% | 267 | 222 | 28 | 259 | 162 | 96 |
| Winterthur, Kantonsspital | 1293 | 523 | 770 | 60% | 157 | 173 | 22 | 33 | 28 | 5 |
| Zürich, Hirslanden Klinik | 2591 | 1320 | 1271 | 49% | 107 | 95 | 9 | 21 | 19 | 2 |
| Zürich, Klinik im Park | 1111 | 606 | 505 | 45% | 39 | 33 | 9 | 26 | 16 | 11 |
| Zürich, Triemli Stadtspital | 2971 | 1557 | 1414 | 48% | 418 | 400 | 52 | 65 | n.a. | n.a. |
| Zürich, Universitätsspital | 3514 | 1746 | 1768 | 50% | 425 | 341 | n.a. | n.a. | n.a. | n.a. |
| Total | 57309 | 29991 | 27318 | 47% | 5923 | 4426 | 667 | 1739 | 1164 | 257 |
CA = coronary angiography; CTO = chronic total occlusion; n.a. = not available; NST-ACS = non-ST-segment elevation acute coronary syndromes; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction
Table 3 Characteristics of the coronary interventions: access and stenting.
| Centre | Radial access for CA | Radial access for PCI | Radial access for CA (rate) | Radial access for PCI (rate) | BMS | DES | Self-expandable stents (DES or BMS) | Bioabsorbable scaffolds (Absorb, Magmaris, etc.) | Bifurcation dedicated stents |
|---|---|---|---|---|---|---|---|---|---|
| Aarau, Hirslanden Klinik | 272 | 125 | 47% | 61% | 1 | 195 | – | – | – |
| Aarau, Kantonsspital | 946 | 546 | 42% | 56% | – | 934 | – | – | – |
| Baden, Kantonsspital | 171 | 137 | 31% | 83% | – | 161 | – | 5 | – |
| Basel, St. Claraspital | 79 | 30 | 16% | 15% | – | 191 | – | – | – |
| Basel, Universitätsspital | 1701 | 750 | 68% | 62% | – | 1128 | 23 | – | – |
| Bern, Klinik Beau-Site | n.a. | 248 | n.a. | 36% | – | 857 | – | – | – |
| Bern, Lindenhofspital | 1161 | 648 | 83% | 88% | – | 718 | – | – | 243 |
| Bern, Universitätsspital und Tiefenau | 3985 | 1895 | 61% | 69% | 1 | 2499 | – | 1 | – |
| Biel, Spitalzentrum | 473 | 243 | 52% | 64% | – | 371 | – | – | – |
| Brig, Centre de Cardiologie du Valais | 330 | 139 | 98% | 99% | – | 135 | – | – | – |
| Chur, Kantonsspital Graubünden | 776 | 410 | 69% | 63% | – | 1004 | – | – | – |
| Frauenfeld, Kantonsspital Thurgau | 476 | 221 | 69% | 72% | – | 295 | 1 | – | – |
| Fribourg, Hôpital cantonal | 349 | 162 | 16% | 15% | 2 | 1074 | – | – | – |
| Genf, Clinique des Grangettes | 539 | 289 | 95% | 92% | – | 545 | – | – | – |
| Genf, Hôpital de la Tour | 651 | 253 | 79% | 81% | – | 293 | – | – | – |
| Genf, Hôpitaux universitaires | 1670 | 821 | 88% | 92% | 2 | 794 | – | n.a. | n.a. |
| Genolier, Clinique de Genolier | 165 | 148 | 38% | 61% | – | 221 | – | – | – |
| Kreuzlingen, Herz-Neuro-Zentrum Bodensee | 838 | 671 | 68% | 102% | – | 649 | – | – | – |
| Lachen, Spital | 163 | 52 | 86% | 87% | – | 60 | – | – | – |
| Lausanne, Centre hospitalier universitaire vaudois | 1573 | 785 | 70% | 77% | 6 | 956 | – | 6 | – |
| Lausanne, Clinique Cecil | 844 | 537 | 40% | 62% | 7 | 804 | – | – | – |
| Lausanne, Clinique de la Source | 716 | 351 | 69% | 68% | 34 | 484 | – | – | – |
| Liestal, Kantonsspital Baselland | 833 | 460 | 89% | 87% | – | 487 | – | 23 | – |
| Lugano, Cardiocentro Ticino | 913 | 932 | 38% | 68% | – | 1338 | 10 | 17 | – |
| Luzern, Kantonsspital | 1542 | 1179 | 47% | 83% | – | 1421 | 8 | – | – |
| Luzern, Klinik St. Anna | 390 | 331 | 33% | 45% | – | 590 | – | 4 | – |
| Morges, Hôpital | 176 | 161 | 37% | 74% | 1 | 209 | – | – | – |
| Pfäffikon, Cardiance Clinic | 74 | 43 | 19% | 21% | – | 201 | – | – | – |
| Sion, Hôpital du Valais | 1120 | 542 | 78% | 79% | – | 680 | – | – | – |
| Solothurn, Bürgerspital | 371 | 176 | 27% | 24% | – | 697 | – | – | – |
| St. Gallen, Kantonsspital | 2201 | 1198 | 80% | 91% | – | 1314 | 11 | 3 | – |
| Winterthur, Kantonsspital | 752 | 412 | 58% | 54% | – | 724 | 7 | – | – |
| Zürich, Hirslanden Klinik | 657 | 695 | 25% | 55% | 1 | 1192 | 2 | – | – |
| Zürich, Klinik im Park | 521 | 274 | 47% | 54% | – | 437 | – | – | – |
| Zürich, Triemli Stadtspital | 1200 | 1000 | 40% | 71% | – | 1412 | 2 | – | – |
| Zürich, Universitätsspital | n.a. | n.a. | n.a. | n.a. | – | 3512 | – | 2 | n.a. |
| Total | 28628 | 16864 | 56% | 66% | 55 | 28582 | 64 | 61 | 243 |
BMS = bare metal stents; CA = coronary angiography; DES = drug-eluting stent; n.a. = not available; PCI = percutaneous coronary intervention
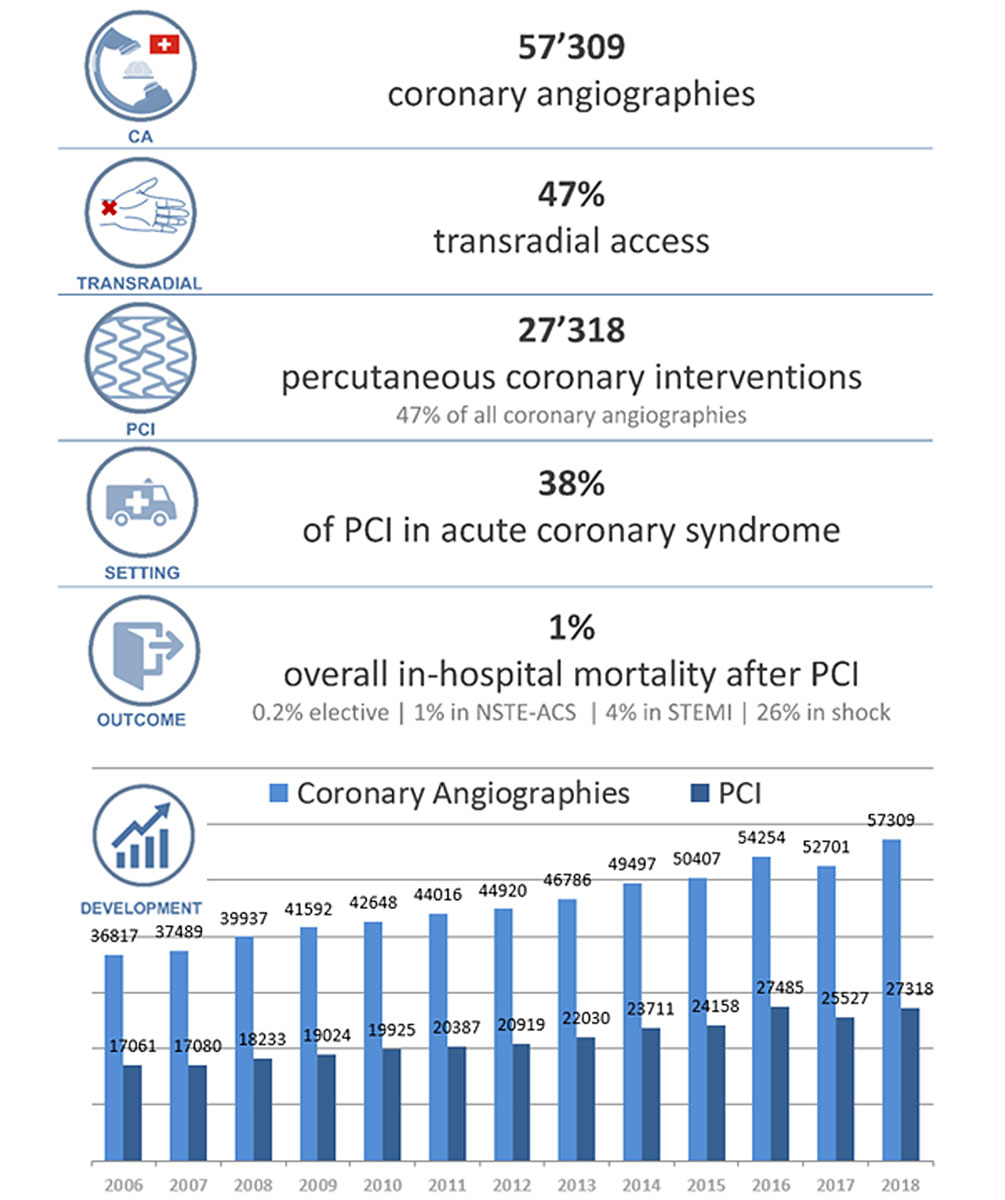
Figure 2 Coronary interventions in Switzerland: summary 2018 and development 2006–2018. CA = coronary angiography; PCI = percutaneous coronary intervention
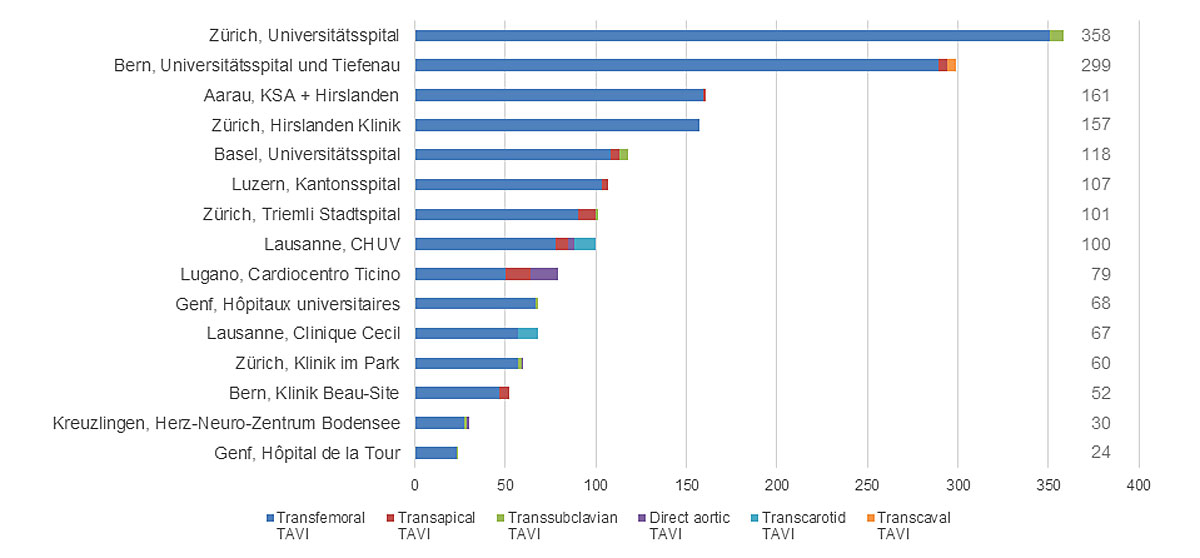
Figure 3 Transcatheter aortic valve implantations (TAVI) during the year 2018 in Switzerland.
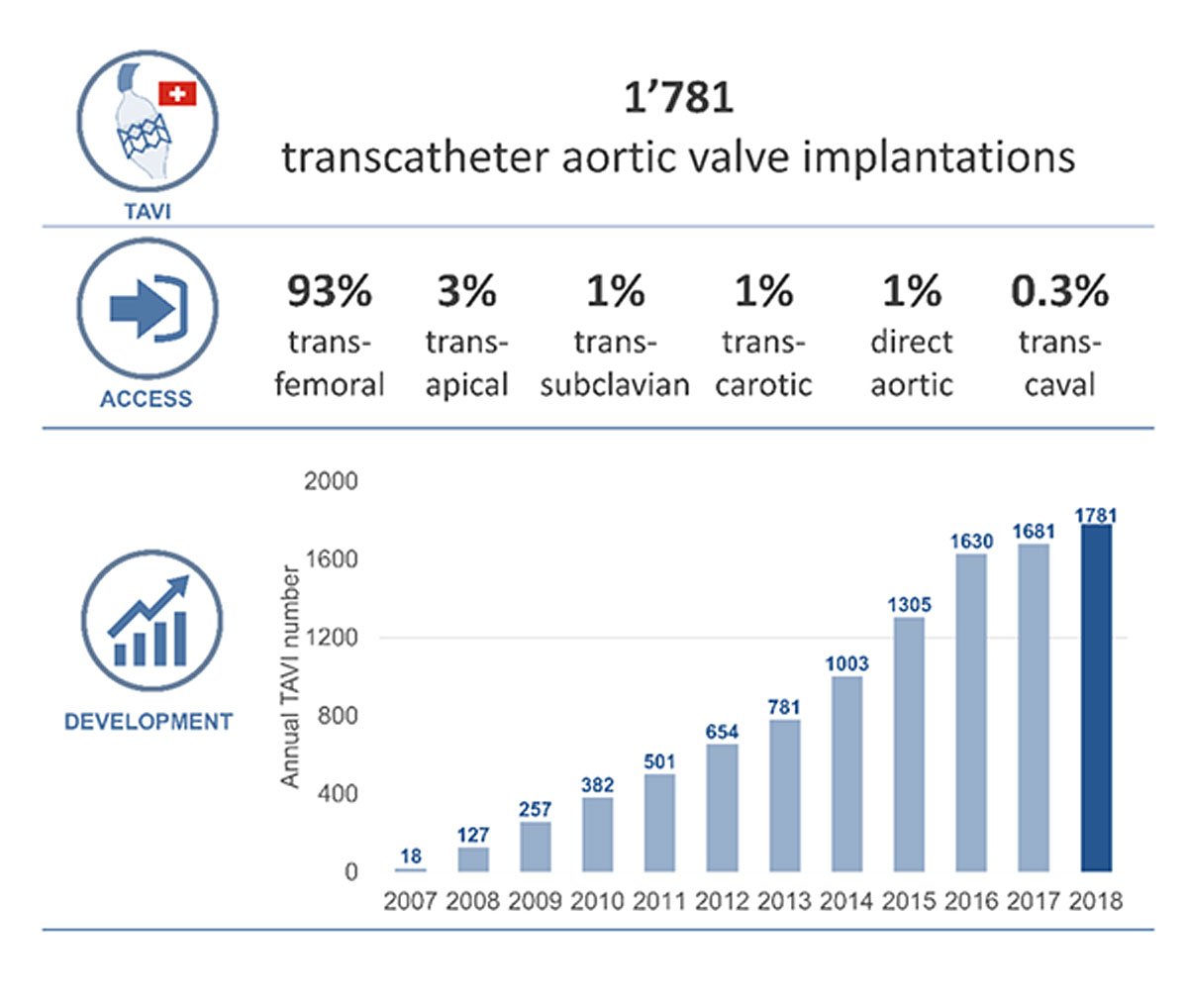
Figure 4 Transcatheter aortic valve implantations in Switzerland: summary 2018 and development 2007–2018.
Among all stents, the drug-eluting stent (DES) was almost always the stent type applied (99%). Bare metal stents (BMSs), bioresorbable or self-expandable stents were used in a minority of patients only (0.2, 0.2 and 0.2%, respectively). PCI in chronic total occlusion (CTO) was performed in 6.4% of all PCI cases (1739 patients), whereas the majority of CTO cases the procedure was done by the antegrade route (82% of CTO cases; table 3).
Emergency interventions in patients with a STEMI accounted for 16% of PCI procedures, whereas 22% of patients presented with NSTE-ACS. PCI for cardiogenic shock accounted for 2.4% of all PCI cases (table 2). In 2018, mechanical support systems were used in 494 patients (1.8% of PCI cases; Impella [Abiomed Inc, Danvers MA] in 231 patients, intra-aortic balloon pumps in 176 patients and extracorporeal membrane oxygenation in 87 patients). Pericardial drainage was performed in 322 patients. A catheter-based therapy of pulmonary embolism (e.g., EKOS) was performed in 98 patients (table 4).
Table 4 Characteristics of the coronary interventions: revascularisation techniques (other than balloon angioplasty), pressure measurements and mechanical support systems.
| Centre | Rotablator (number of cases) | Thrombus aspiration | Distal protection device | FFR | iFR | IVUS | OCT | IABP | Impella | ECMO |
|---|---|---|---|---|---|---|---|---|---|---|
| Aarau, Hirslanden Klinik | – | – | – | – | 20 | – | – | 1 | – | – |
| Aarau, Kantonsspital | 18 | – | 8 | 46 | 70 | 9 | 47 | 1 | 14 | – |
| Baden, Kantonsspital | – | 4 | 5 | 22 | – | – | – | – | – | – |
| Basel, St. Claraspital | 5 | 99 | – | 44 | 20 | 40 | 40 | 6 | – | – |
| Basel, Universitätsspital | 24 | 57 | 2 | 120 | – | 19 | 28 | – | 41 | 2 |
| Bern, Klinik Beau–Site | 8 | 8 | – | 94 | – | – | – | 1 | – | – |
| Bern, Lindenhofspital | 4 | – | – | – | – | – | – | – | – | – |
| Bern, Universitätsspital und Tiefenau | 40 | 201 | 4 | 222 | 9 | 22 | 217 | 9 | 45 | 25 |
| Biel, Spitalzentrum | 4 | 14 | – | 22 | – | – | – | – | 2 | – |
| Brig, Centre de Cardiologie du Valais | – | – | – | 57 | – | – | 10 | – | – | – |
| Chur, Kantonsspital Graubünden | 7 | 55 | – | 11 | 62 | 4 | 11 | 5 | – | – |
| Frauenfeld, Kantonsspital Thurgau | – | – | – | 21 | 34 | – | 6 | – | – | – |
| Fribourg, Hôpital cantonal | 11 | 29 | – | 77 | – | 13 | 58 | 9 | – | 3 |
| Genf, Clinique des Grangettes | 5 | – | 3 | 74 | – | – | 11 | – | – | – |
| Genf, Hôpital de la Tour | 11 | 14 | 6 | 71 | 2 | 11 | – | 6 | – | – |
| Genf, Hôpitaux universitaires | 16 | 40 | 2 | 2 | 239 | 40 | 35 | 5 | – | 5 |
| Genolier, Clinique de Genolier | 5 | – | 1 | 108 | – | – | 17 | – | – | – |
| Kreuzlingen, Herz–Neuro–Zentrum Bodensee | – | – | – | 15 | 145 | 3 | – | – | – | – |
| Lachen, Spital | – | – | – | 15 | – | 3 | – | – | – | – |
| Lausanne, Centre hospitalier universitaire vaudois | 28 | 149 | 6 | 195 | – | 32 | 68 | 10 | – | 13 |
| Lausanne, Clinique Cecil | 1 | 2 | – | 115 | – | – | – | 1 | – | 1 |
| Lausanne, Clinique de la Source | – | 11 | – | 149 | – | – | – | – | – | – |
| Liestal, Kantonsspital Baselland | 11 | 4 | 3 | 47 | – | – | 32 | – | 4 | – |
| Lugano, Cardiocentro Ticino | 3 | 87 | 15 | 105 | 248 | 49 | 81 | 16 | 3 | 11 |
| Luzern, Kantonsspital | 2 | 284 | 1 | 197 | – | 10 | 90 | 32 | 47 | 4 |
| Luzern, Klinik St. Anna | 8 | – | – | 112 | 2 | 23 | – | 2 | 4 | – |
| Morges, Hôpital | 5 | 1 | 2 | 29 | – | – | 9 | – | – | – |
| Pfäffikon, Cardiance Clinic | – | 1 | – | 1 | 22 | 1 | – | – | – | – |
| Sion, Hôpital du Valais | – | 22 | – | 121 | – | – | 12 | 10 | – | 3 |
| Solothurn, Bürgerspital | 6 | 9 | 1 | 135 | – | – | – | – | – | – |
| St. Gallen, Kantonsspital | 114 | 145 | 3 | 141 | 122 | 56 | 16 | 22 | 11 | 10 |
| Winterthur, Kantonsspital | 10 | 20 | – | 25 | 129 | 27 | – | – | 9 | 3 |
| Zürich, Hirslanden Klinik | 5 | – | 5 | – | 282 | 53 | 4 | 13 | 5 | 4 |
| Zürich, Klinik im Park | 2 | 1 | – | 8 | 167 | – | – | 10 | – | 3 |
| Zürich, Triemli Stadtspital | 5 | 25 | 12 | 93 | – | – | 20 | 17 | 16 | – |
| Zürich, Universitätsspital | 45 | n.a. | n.a. | 75 | n.a. | 119 | 55 | n.a. | 30 | n.a. |
| Total | 403 | 1282 | 79 | 2569 | 1573 | 534 | 867 | 176 | 231 | 87 |
ECMO = extracorporeal membrane oxygenation; FFR = fractional flow reserve; IABP = intra–aortic balloon counterpulsation; iFR = instant wave free ratio; IVUS = intravascular ultrasound; n.a. = not available; OCT = intravascular optical coherence tomography
Intracoronary pressure measurements (fractional flow reserve [FFR] or instant wave free ration [iFR]) were made in 2569 (9.4%) and 1573 (5.8%) patients, respectively. Intravascular ultrasound (IVUS) and intravascular optical coherence tomography (OCT) was performed in 534 (1.9%) and in 867 (3.2%) patients, respectively. Distal protection devices were used in 79 patients (0.3% of PCI cases). Revascularisation techniques other than balloon angioplasty included rotablation (403 patients, 1.5% of PCI cases) and thrombus aspiration (1282 patients, 4.7%; table 4).
The mean overall in-hospital mortality rate after PCI was 1.0%. The mortality rate after PCI for stable CAD was 0.2%, after PCI for NSTE-ACS 1.2%, after PCI for STEMI 4.3% and after PCI for cardiogenic shock or cardiac arrest 26.2% (fig. 2).
Since 2006, almost all Swiss interventional centres report their data to the Swiss Working Group Interventional Cardiology of the Swiss Society of Cardiology. Since 2010, the number of facilities with a cardiac catheterisation laboratory increased from 33 to 36, corresponding to a total increase in cardiac catheterisation rooms from 50 in 2011 to 60 in 2018. The number of facilities with on-site cardiac surgery remained stable at 16 centres. Accordingly, the number of operators performing PCI rose from 144 in 2011 to 224 in 2018. The evolution of cases of CA and PCI is shown in figure 2. The ratio of PCI to CA remained virtually the same over the years (47% in 2010 and 47% in 2018) [8]. The percentage of radial access increased steadily from 15% in 2010 to 35% in 2014, and reached now 47% in 2018, reflecting the adoption of new recommendations. The number of PCIs per 100,000 inhabitants increased steadily from 254/100,000 in 2010 to 320/100,000 in 2018. Mortality rates were comparable to reports from previous years [8].
Eleven years after its first introduction in Switzerland in 2007, TAVI continued to increase over the years with a slight flattening since 2016 (from 382 procedures performed in 11 centres in 2010 to 1781 cases in 15 centres in 2018) (figs 3 and 4 ). Most cases currently are performed by the transfemoral route (1663 patients, 93% of all cases).Access via the transapical (52 patients, 1.9%), trans-subclavian (19 patients, 1.1%) trans-carotid (23 patients, 1.3%), direct aortic (20 patients, 1.1%) and transcaval (5 patients, 0.3%) routes are less often used (figs 3 and 4 , table 5).
Table 5 Structural interventions: aortic valve.
| Centre | Aortic valvuloplasty without percutaneous valve replacement | TAVI | Trans-femoral TAVI | Trans-apical TAVI | Trans-subclavian TAVI | Direct aortic TAVI | Trans-carotid TAVI | Trans-caval TAVI | Use of embolic protection device during TAVI |
|---|---|---|---|---|---|---|---|---|---|
| Aarau, Hirslanden Klinik | – | 161 | 159 | 2 | – | – | – | – | – |
| Aarau, Kantonsspital | – | – | – | – | – | – | – | – | – |
| Baden, Kantonsspital | – | – | – | – | – | – | – | – | – |
| Basel, St. Claraspital | 1 | – | – | – | – | – | – | – | – |
| Basel, Universitätsspital | 2 | 118 | 108 | 5 | 5 | – | – | – | 2 |
| Bern, Klinik Beau-Site | – | 52 | 47 | 5 | – | – | – | – | – |
| Bern, Lindenhofspital | – | – | – | – | – | – | – | – | – |
| Bern, Universitätsspital und Tiefenau | – | 299 | 289 | 5 | – | – | – | 5 | 2 |
| Biel, Spitalzentrum | – | – | – | – | – | – | – | – | – |
| Brig, Centre de Cardiologie du Valais | – | – | – | – | – | – | – | – | – |
| Chur, Kantonsspital Graubünden | – | – | – | – | – | – | – | – | – |
| Frauenfeld, Kantonsspital Thurgau | – | – | – | – | – | – | – | – | – |
| Fribourg, Hôpital cantonal | – | – | – | – | – | – | – | – | – |
| Genf, Clinique des Grangettes | – | – | – | – | – | – | – | – | – |
| Genf, Hôpital de la Tour | 1 | 24 | 23 | – | 1 | – | – | – | – |
| Genf, Hôpitaux universitaires | – | 68 | 67 | – | 1 | – | – | – | 5 |
| Genolier, Clinique de Genolier | – | – | – | – | – | – | – | – | – |
| Kreuzlingen, Herz-Neuro-Zentrum Bodensee | – | 30 | 27 | – | 2 | 1 | – | – | – |
| Lachen, Spital | – | – | – | – | – | – | – | – | – |
| Lausanne, Centre hospitalier universitaire vaudois | – | 100 | 78 | 7 | – | 3 | 12 | – | – |
| Lausanne, Clinique Cecil | 1 | 67 | 57 | – | – | – | 11 | – | – |
| Lausanne, Clinique de la Source | – | – | – | – | – | – | – | – | – |
| Liestal, Kantonsspital Baselland | – | – | – | – | – | – | – | – | – |
| Lugano, Cardiocentro Ticino | 4 | 79 | 50 | 14 | – | 15 | – | – | 12 |
| Luzern, Kantonsspital | 5 | 107 | 103 | 4 | – | – | – | – | – |
| Luzern, Klinik St. Anna | – | – | – | – | – | – | – | – | – |
| Morges, Hôpital | – | – | – | – | – | – | – | – | – |
| Pfäffikon, Cardiance Clinic | – | – | – | – | – | – | – | – | – |
| Sion, Hôpital du Valais | – | – | – | – | – | – | – | – | – |
| Solothurn, Bürgerspital | – | – | – | – | – | – | – | – | – |
| St. Gallen, Kantonsspital | – | – | – | – | – | – | – | – | n.a. |
| Winterthur, Kantonsspital | – | – | – | – | – | – | – | – | – |
| Zürich, Hirslanden Klinik | – | 157 | 157 | – | – | – | – | – | – |
| Zürich, Klinik im Park | 3 | 60 | 57 | – | 2 | 1 | – | – | – |
| Zürich, Triemli Stadtspital | – | 101 | 90 | 10 | 1 | – | – | – | – |
| Zürich, Universitätsspital | – | 358 | 351 | – | 7 | – | – | – | n.a. |
| Total | 17 | 1781 | 1663 | 52 | 19 | 20 | 23 | 5 | 21 |
n.a. = not available; TAVI = transcatheter aortic valve implantation
Nine years after its introduction in 2009, transcatheter mitral edge-to-edge repair procedures using the Mitraclip device (Abbott Strucural Heart, Santa Clara CA) showed a pronounced increase from 67 cases in 4 centres in 2010 to 382 cases in 14 centres in 2018 (table 6a). Additionally, transcatheter direct mitral annuloplasty using the Cardioband device (Edwards Lifesciences, Irvine CA) was performed in nine patients and indirect mitral annuloplasty using the Carillon device (Cardiac Dimensions, Kirkland, WA) in six patients in two centres in Switzerland. Transcatheter tricuspid interventions (32 patients), pulmonal valvuloplasty (33 patients), and transcatheter pulmonary valve implantations (6 patients) were performed in 8 centres in Switzerland. Detailed information on TAVI and mitral transcatheter edge-to-edge repair procedures performed in Switzerland can be found in the SwissTAVI [9] and MitraSwiss [10] registries.
Table 6 a: Structural interventions: other.
| Centre | Occlusion of para-valvular leakage | Percutaneous transvenous mitral valvuloplasty | Mitral edge-to-edge repair devices (e.g. Mitraclip, Pascal) | Transcatheter direct mitral annuloplasty (e.g. Cardioband, Accucinch) | Transcatheter indirect mitral annuloplasty (e.g. Carillon) | Transcatheter tricuspid valve intervention | PTA / stenting pulmonary artery | Transcatheter pulmonary valvuloplasty | TPVI (e.g. Melody) |
|---|---|---|---|---|---|---|---|---|---|
| Aarau, Hirslanden Klinik | – | – | 11 | – | – | – | – | – | – |
| Aarau, Kantonsspital | – | – | 51 | – | – | – | – | – | – |
| Baden, Kantonsspital | – | – | – | – | – | – | – | – | – |
| Basel, St. Claraspital | – | – | – | – | – | – | – | – | – |
| Basel, Universitätsspital | 2 | 2 | 16 | 3 | – | 1 | – | – | – |
| Bern, Klinik Beau–Site | – | – | – | – | – | – | – | – | – |
| Bern, Lindenhofspital | – | – | – | – | – | – | – | – | – |
| Bern, Universitätsspital und Tiefenau | 13 | 2 | 70 | – | – | 10 | 32 | 5 | 1 |
| Biel, Spitalzentrum | – | – | – | – | – | – | – | – | – |
| Brig, Centre de Cardiologie du Valais | – | – | – | – | – | – | – | – | – |
| Chur, Kantonsspital Graubünden | – | – | – | – | – | – | – | – | – |
| Frauenfeld, Kantonsspital Thurgau | – | – | – | – | – | – | – | – | – |
| Fribourg, Hôpital cantonal | – | – | 9 | – | – | – | – | – | – |
| Genf, Clinique des Grangettes | – | – | – | – | – | – | – | – | – |
| Genf, Hôpital de la Tour | – | – | – | – | – | – | – | – | – |
| Genf, Hôpitaux universitaires | 1 | – | 20 | – | – | – | – | – | – |
| Genolier, Clinique de Genolier | – | – | – | – | – | – | – | – | – |
| Kreuzlingen, Herz–Neuro–Zentrum Bodensee | – | – | 1 | – | – | – | – | – | – |
| Lachen, Spital | – | – | – | – | – | – | – | – | – |
| Lausanne, Centre hospitalier universitaire vaudois | 6 | 5 | 21 | – | – | 1 | 1 | 4 | 3 |
| Lausanne, Clinique Cecil | – | – | – | – | – | – | – | – | – |
| Lausanne, Clinique de la Source | – | – | – | – | – | – | – | – | – |
| Liestal, Kantonsspital Baselland | – | – | – | – | – | – | – | – | – |
| Lugano, Cardiocentro Ticino | – | – | 11 | – | – | 6 | – | – | 1 |
| Luzern, Kantonsspital | 3 | 3 | 36 | – | – | 2 | – | – | – |
| Luzern, Klinik St. Anna | – | – | 6 | – | – | – | – | – | – |
| Morges, Hôpital | – | – | – | – | – | – | – | – | – |
| Pfäffikon, Cardiance Clinic | – | – | – | – | – | – | – | – | – |
| Sion, Hôpital du Valais | – | – | – | – | – | – | – | – | – |
| Solothurn, Bürgerspital | – | – | – | – | – | – | – | – | – |
| St. Gallen, Kantonsspital | 2 | – | – | – | – | – | – | – | – |
| Winterthur, Kantonsspital | – | – | – | – | – | – | – | – | – |
| Zürich, Hirslanden Klinik | 3 | – | 37 | – | – | 5 | – | – | – |
| Zürich, Klinik im Park | – | 1 | 25 | – | – | – | – | – | – |
| Zürich, Triemli Stadtspital | 1 | 1 | 3 | – | – | 1 | – | – | – |
| Zürich, Universitätsspital | 8 | 6 | 65 | 6 | 6 | 6 | – | – | 1 |
| Total | 39 | 20 | 382 | 9 | 6 | 32 | 33 | 9 | 6 |
PTA = percutaneous transluminal angioplasty; TPVI = transcatheter pulmonary valve implantation
We noted an increase in left atrial appendage (LAA) closure from 117 in 2011 to 406 in 2018 and an increase of paravalvular leak closure from 10 in 2011 to 39 in 2018. The number of persistent foramen ovale (PFO) and atrial septal defect (ASD) closures remained roughly stable over the years, with 733 PFO closures in 2010 and 833 in 2018; the corresponding numbers for ASD closures were 142 and 154. Interventional ventricular septal defect (VSD) closures were performed in 11 patients in 2018. TASH, renal denervation and coronary sinus reduction were performed in 34, 11 and 19 cases, respectively, in 2018 (table 6b).
Table 6b Structural interventions: other.
| Centre | Alcohol ablation for septal hypertrophy | Pericardial drainage (ad hoc or scheduled) | Catheter-based therapy of pulmonary embolism | Catheter-based renal sympathetic denervation for treatment of hypertension | Coronary sinus reduction | PFO closure | ASD closure | VSD closure | LAA closure |
|---|---|---|---|---|---|---|---|---|---|
| Aarau, Hirslanden Klinik | – | – | – | – | – | 3 | – | – | 1 |
| Aarau, Kantonsspital | 2 | – | – | – | – | 58 | 7 | – | 47 |
| Baden, Kantonsspital | – | – | – | – | – | – | – | – | – |
| Basel, St. Claraspital | – | 6 | – | – | – | – | – | – | – |
| Basel, Universitätsspital | 1 | 25 | 2 | – | 2 | 32 | 5 | – | 20 |
| Bern, Klinik Beau–Site | – | – | – | – | – | 3 | 7 | – | 1 |
| Bern, Lindenhofspital | – | 9 | 1 | – | – | 10 | 20 | – | – |
| Bern, Universitätsspital und Tiefenau | 4 | 43 | 57 | 1 | – | 176 | 28 | 1 | 84 |
| Biel, Spitalzentrum | – | 3 | – | – | – | 6 | – | – | – |
| Brig, Centre de Cardiologie du Valais | – | – | – | – | – | 0 | – | – | – |
| Chur, Kantonsspital Graubünden | – | 0 | – | – | – | 4 | – | 1 | – |
| Frauenfeld, Kantonsspital Thurgau | – | 0 | – | – | – | 12 | – | – | – |
| Fribourg, Hôpital cantonal | 3 | 19 | 3 | – | 1 | 30 | 10 | – | 10 |
| Genf, Clinique des Grangettes | – | – | – | – | – | 3 | – | – | – |
| Genf, Hôpital de la Tour | – | 7 | – | – | – | 10 | 3 | – | 3 |
| Genf, Hôpitaux universitaires | 3 | 26 | 32 | – | – | 40 | 1 | – | 17 |
| Genolier, Clinique de Genolier | – | 1 | – | 1 | – | 3 | – | – | – |
| Kreuzlingen, Herz–Neuro–Zentrum Bodensee | – | 2 | – | – | – | 7 | – | – | – |
| Lachen, Spital | – | 5 | – | – | – | 6 | – | – | – |
| Lausanne, Centre hospitalier universitaire vaudois | 1 | 20 | – | 2 | – | 26 | 18 | 3 | 2 |
| Lausanne, Clinique Cecil | – | 10 | – | – | – | 10 | – | – | 2 |
| Lausanne, Clinique de la Source | 2 | 12 | – | – | 1 | 6 | – | – | – |
| Liestal, Kantonsspital Baselland | 2 | 10 | 2 | – | – | 13 | – | – | – |
| Lugano, Cardiocentro Ticino | – | 23 | – | – | 7 | 15 | 5 | – | 12 |
| Luzern, Kantonsspital | 3 | 36 | 1 | – | 4 | 34 | 2 | 1 | 13 |
| Luzern, Klinik St. Anna | – | 2 | – | 1 | – | 4 | – | 1 | 7 |
| Morges, Hôpital | – | 1 | – | – | – | 2 | – | – | – |
| Pfäffikon, Cardiance Clinic | 1 | 1 | – | – | – | 7 | 2 | – | 1 |
| Sion, Hôpital du Valais | – | 15 | – | 1 | – | 11 | 2 | – | 2 |
| Solothurn, Bürgerspital | – | 3 | – | 1 | – | 17 | – | – | 10 |
| St. Gallen, Kantonsspital | 2 | 15 | – | – | – | 27 | 3 | – | 7 |
| Winterthur, Kantonsspital | – | 4 | – | – | – | 21 | – | – | – |
| Zürich, Hirslanden Klinik | – | 7 | – | – | – | 35 | 10 | – | 24 |
| Zürich, Klinik im Park | 5 | 8 | – | 4 | – | 39 | 4 | – | 28 |
| Zürich, Triemli Stadtspital | 5 | 9 | – | – | 2 | 56 | 8 | – | 29 |
| Zürich, Universitätsspital | n.a. | n.a. | n.a. | n.a. | 2 | 107 | 19 | 4 | 86 |
| Total | 34 | 322 | 98 | 11 | 19 | 833 | 154 | 11 | 406 |
| ASD = atrial septal defect; LAA = left atrial appendage; n.a. = not available; PFO = patent foramen ovale; VSD = ventricular septal defect | |||||||||
Limitations of this report include the fact that the survey was based on aggregate data submitted by the centres on a voluntary basis and not subjected to monitoring. While all centres provided data for this survey, not all information was available for all items in every centre.
The data collected in 2018 show a high and adequate number of diagnostic and therapeutic coronary procedures in comparison with other countries [11, 12], as well as a significant qualitative leap in advanced intracoronary diagnostic techniques as compared to with from previous years [5–8]. The increasing dominance of the radial approach and the high rate of PCI as treatment for acute myocardial infarction and ischaemic coronary artery disease are clear indicators of the quality of the Swiss interventional activity. Furthermore, there has been a marked increase in the number of procedures for structural heart disease over the last 10 years, for both TAVI and percutaneous mitral valve repair, which incorporates and reflects current guidelines and European standards.
We are indebted to all representatives of the catheterisation laboratories participating in this survey. Furthermore, we acknowledge the effort of all the centres which collected the survey data and completed the questionnaires.
TN has received speaker honoraria/consulting honoraria from Beckman Coulter, Bayer, Ortho Clinical Diagnostics and Orion Pharma. RT has received research support from the Swiss National Science Foundation (P300PB_167803), the Swiss Heart Foundation, the Swiss Society of Cardiology, the University Hospital of Basel, as well as speaker honoraria/consulting honoraria from Roche Diagnostics, Abbott Diagnostics, Siemens, Singulex and Brahms. LR reports research grants by Abbott, Biotronik, Boston Scientific, Heartflow, Sanofi and Regeneron and speaker fees by Abbott, AstraZeneca, Amgen, CSL Behring, Occlutech, Sanofi and Vifor. RJ has received speaker honoraria from B. Braun Melsungen AG and Cardionovum and research support from B. Braun Melsungen AG. FN has acted as consultant to Edwards Lifesciences. OM Has received honoraria from Abbott and Edwards Lifesciences. Other authors declare that they have no conflict of interest related to this study.
1 Windecker S , Kolh P , Alfonso F , Collet JP , Cremer J , et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541–619. doi:.https://doi.org/10.1093/eurheartj/ehu278
2 Nishimura RA , Otto CM , Bonow RO , Carabello BA , Erwin JP, 3rd , Fleisher LA , et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135(25):e1159–95. doi:.https://doi.org/10.1161/CIR.0000000000000503
3 Baumgartner H , Falk V , Bax JJ , De Bonis M , Hamm C , Holm PJ , et al.; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739–91. doi:.https://doi.org/10.1093/eurheartj/ehx391
4 Meier B . [Local development of coronary angioplasty]. Schweiz Med Wochenschr. 1989;119(30):1033–9. German.
5 Windecker S , Roffi M , Pedrazzini G , Rickli H , Maeder T , Kaiser A , et al. Interventional Cardiology in Switzerland during the Year 2007. Cardiovasc Med. 2010;13(01):18–24. doi:https://doi.org/10.4414/cvm.2010.01466
6 Windecker S , Pedrazzini G , Roffi M , Rickli H , Maeder T , Kaiser A , et al. Interventional cardiology in Switzerland during the years 2008 and 2009. Cardiovasc Med. 2010;13(12):370–5. doi:.https://doi.org/10.4414/cvm.2010.01544
7 Pedrazzini G , Roffi M , Cook S , Corti R , Wenaweser P , Rickli H , et al. Interventional cardiology in Switzerland during the year 2010. Cardiovasc Med. 2012;15(02):48–53. doi:.https://doi.org/10.4414/cvm.2012.01647
8 Rigamonti F , Fahrni G , Maeder M , Cook S , Weilenmann D , Wenaweser P , et al. Switzerland: coronary and structural heart interventions from 2010 to 2015. EuroIntervention. 2017;13(Z):Z75–9. doi:.https://doi.org/10.4244/EIJ-D-16-00828
9 Wenaweser P , Stortecky S , Heg D , Tueller D , Nietlispach F , Falk V , et al. Short-term clinical outcomes among patients undergoing transcatheter aortic valve implantation in Switzerland: the Swiss TAVI registry. EuroIntervention. 2014;10(8):982–9. doi:.https://doi.org/10.4244/EIJV10I8A166
10 Sürder D , Pedrazzini G , Gaemperli O , Biaggi P , Felix C , Rufibach K , et al. Predictors for efficacy of percutaneous mitral valve repair using the MitraClip system: the results of the MitraSwiss registry. Heart. 2013;99(14):1034–40. doi:.https://doi.org/10.1136/heartjnl-2012-303105
11 Pereira H , Teles RC , Costa M , da Silva PC , Ferreira RC , da Gama Ribeiro V , et al., Registo Nacional de Cardiologia de Intervenc¸ão. Evolução da intervenção coronária percutânea entre 2004‐2013. Atividade em Portugal segundo o Registo Nacional de Cardiologia de Intervenção [Trends in percutaneous coronary intervention from 2004 to 2013 according to the Portuguese National Registry of Interventional Cardiology]. Rev Port Cardiol. 2015;34(11):673–81. English, Portugese. doi:.https://doi.org/10.1016/j.repc.2015.06.005
12 Cid Álvarez AB , Rodríguez Leor O , Moreno R , Pérez de Prado A . Spanish Cardiac Catheterization and Coronary Intervention Registry. 27th Official Report of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (1990-2017). Rev Esp Cardiol (Engl Ed). 2018;71(12):1036–46. doi:.https://doi.org/10.1016/j.rec.2018.09.009
Contributed equally to the manuscript
The authors designed the investigation, gathered and analysed the data, vouch for the data and analysis, wrote the paper, and decided to submit it for publication. TN, RT and RJ had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors have read and approved the manuscript. The manuscript and its contents have not been published previously and are not being considered for publications elsewhere in whole or in part in any language, including publicly accessible web sites or e-print servers.
TN has received speaker honoraria/consulting honoraria from Beckman Coulter, Bayer, Ortho Clinical Diagnostics and Orion Pharma. RT has received research support from the Swiss National Science Foundation (P300PB_167803), the Swiss Heart Foundation, the Swiss Society of Cardiology, the University Hospital of Basel, as well as speaker honoraria/consulting honoraria from Roche Diagnostics, Abbott Diagnostics, Siemens, Singulex and Brahms. LR reports research grants by Abbott, Biotronik, Boston Scientific, Heartflow, Sanofi and Regeneron and speaker fees by Abbott, AstraZeneca, Amgen, CSL Behring, Occlutech, Sanofi and Vifor. RJ has received speaker honoraria from B. Braun Melsungen AG and Cardionovum and research support from B. Braun Melsungen AG. FN has acted as consultant to Edwards Lifesciences. OM Has received honoraria from Abbott and Edwards Lifesciences. Other authors declare that they have no conflict of interest related to this study.