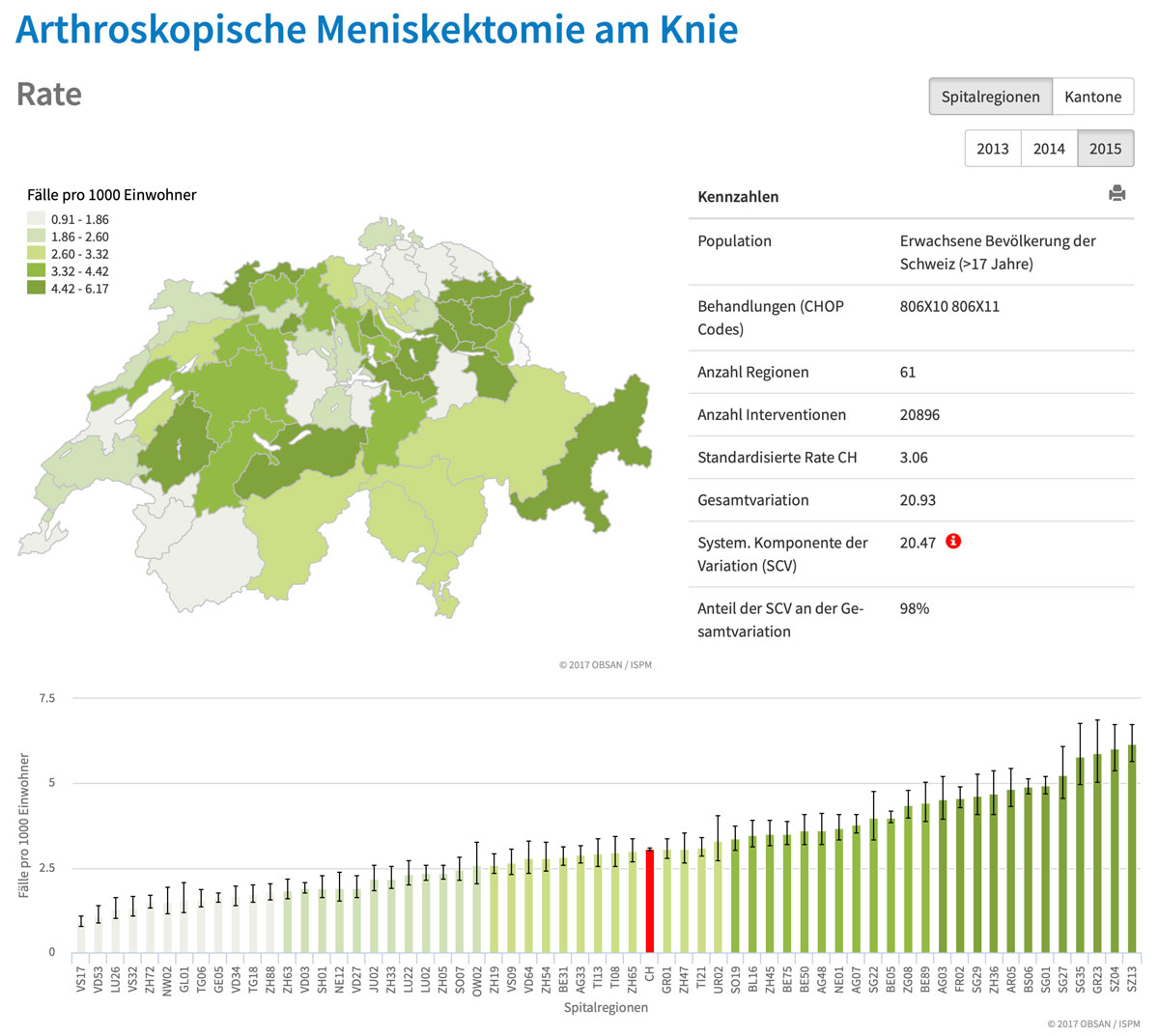
Figure 1 Rate of arthroscopic meniscectomies of the knee across the different healthcare regions of Switzerland (cases per 1000 inhabitants). Source: http://versorgungsatlas.ch
DOI: https://doi.org/10.4414/smw.2019.20029
How do we assess the quality of clinical care for our patients, institutions and an entire country? This is an essential question not only to ensure excellence in clinical medicine, but also to potentially provide means for benchmarking, as well as directing incentives for reimbursement towards an augmentation of value for the patient, rather than just volume [1].
However, this is a complicated task, as no universally accepted metric is available to address this issue. It is indeed quite difficult to measure the quality of clinical care at the level of individual patients, which is currently often assessed with metrics concerning patient satisfaction; this, however, is mostly driven by nonmedical factors. At the hospital level we might be tempted to measure outcomes, such as mortality, which might lead to de-incentivising care for severely sick patients and hinder the shift from curative to palliative treatments.
This challenge becomes even more difficult when we try to assess the quality of the entire healthcare system, where both the quality and the appropriateness of care has to be evaluated, the latter aspect alluding to over- and underuse of diagnostic and therapeutic procedures.
One elegant approach to tackle this was introduced by Elliott S. Fisher, who looked at variations of care in the US [2]. Indeed, this approach is based on the simple assumption that variations of care across healthcare regions of a nation should not be exceedingly high, since this implies that either one region is doing too much or the other is doing too little – both cannot be right. Thanks to the support of the Swiss Academy of Medical Sciences, such an atlas, which is curated by Obsan and the Institute of Social and Preventive Medicine in Bern, has now become available also for Switzerland [3]. Using this freely available tool it is quite impressive to see the large variation of care, such as for certain orthopaedic (fig. 1) or cardiological (fig. 2) procedures, which raises the question of whether we truly have one of the very best healthcare systems worldwide.
Figure 1 Rate of arthroscopic meniscectomies of the knee across the different healthcare regions of Switzerland (cases per 1000 inhabitants). Source: http://versorgungsatlas.ch
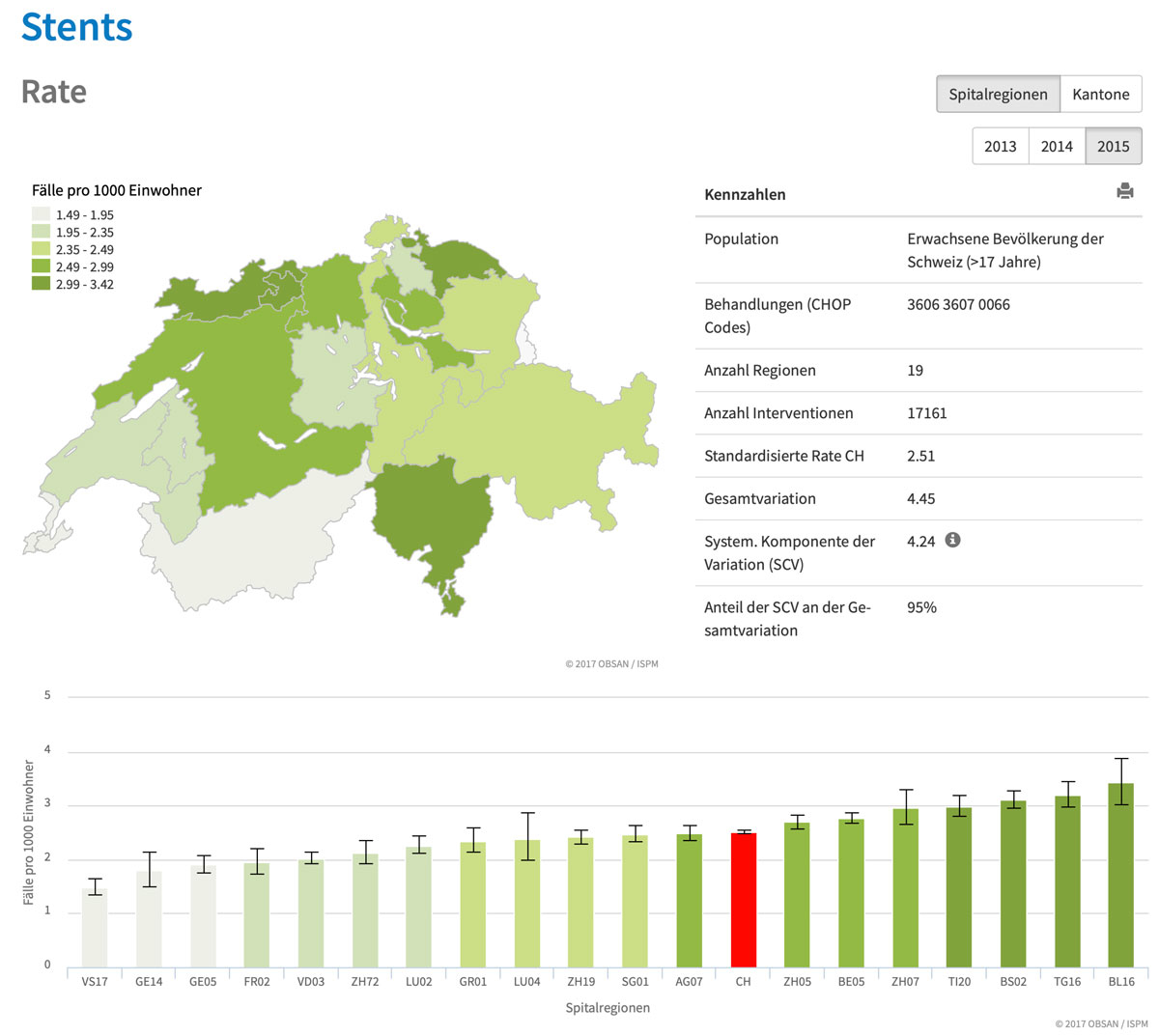
Figure 2 Rate of coronary stent placement across the different healthcare regions of Switzerland (cases per 1000 inhabitants). Source: http://versorgungsatlas.ch
Whereas these analyses can be applied to the use of diagnostic and therapeutic procedures, it is much more complicated to assess the quality of medical diagnoses [4]. Brutsche et al. used geographic variations of a parameter termed the “diagnostic diversity index” (DDI) as a potential indicator for institutional and regional healthcare quality [5]. This question is of great relevance, since diagnostic errors are estimated to occur in up to 15% of all clinical encounters in the US [6]. In their paper, published in the Swiss Medical Weekly [5], the authors assumed that the coding of more detailed and refined diagnoses is more likely to reflect the true diversity of diseases in a population, hence indicating more accurate diagnosis and treatment. In this perspective, a large degree of diagnostic diversity is regarded as an indicator for a high level of diagnostic precision and, by inference, treatment. In order to address this question, the datasets from nearly 10 million hospitalised cases from 2009–2015 in Swiss hospitals were analysed and the DDI was calculated for different healthcare regions and institutions in Switzerland. The authors show a strong association between the case load and number of inhabitants of a healthcare region with the DDI. Specifically, a case load of over 7000 hospitalisations per year and a catchment area of >350,000 inhabitants was associated with a high DDI, hence indicating a higher degree of diagnostic accuracy.
While this approach is conceptually quite elegant, several questions and limitations need to be considered:
In summary, the fact that we have considerable variations of care for treatments and procedures in Switzerland, as shown by the Obsan Atlas, as well as the findings of this study, that relevant variations in the precision of diagnostic classification exist in Switzerland, we are not easily reassured that our healthcare system is homogenously performing at the very best level possible. Hence, these findings need to be addressed seriously by all players in our healthcare system and the focus should not only be placed on the over- or underuse of treatments and procedures, but also on the quality and the timeliness of medical diagnosis [4].
No financial support and no other potential conflict of interest relevant to this article was reported.
1 Porter ME . What is value in health care? N Engl J Med. 2010;363(26):2477–81. doi:.https://doi.org/10.1056/NEJMp1011024
2The Dartmouth Atlas of Helath Care. http://www.dartmouthatlas.org (accessed on November 29th, 2018)
3Schweizer Atlas der Gesundheitsversorgung. http://versorgungsatlas.ch/index.php/de/ (accessed on November 29th, 2018)
4Balogh EP, Miller BT, Ball JR, eds. Improving Diagnosis in Health Care. National Academies Press; 2016.
5 Brutsche M , Rassouli F , Gallion H , Kalra S , Roger VL , Baty F . Diagnostic diversity - an indicator of institutional and regional healthcare quality. Swiss Med Wkly. 2018;148:w14691. doi:.https://doi.org/10.4414/smw.2018.14691
6 Singh H , Meyer AN , Thomas EJ . The frequency of diagnostic errors in outpatient care: estimations from three large observational studies involving US adult populations. BMJ Qual Saf. 2014;23(9):727–31. doi:.https://doi.org/10.1136/bmjqs-2013-002627
No financial support and no other potential conflict of interest relevant to this article was reported.